[Diagnostic Stewardship: Wissen und Einstellungen von Hygienefachpersonal]
Sebastian Schulz-Stübner 1,2,3Teresa Tamayo 1
1 German Consulting Center for Infection Prevention and Control, Freiburg i.Brsg., Germany
2 Clinic for Anesthesiology and Critical Care, University Medical Center Freiburg, University Freiburg, Freiburg i. Brsg., Germany
3 University of Education, Freiburg i. Brsg., Germany
Zusammenfassung
Einleitung: In den letzten Jahren hat das so genannte Diagnostic Stewardship im Rahmen von Antibiotic Stewardship- und Infektionskontrollprogrammen weltweit an Bedeutung gewonnen. Die spezifische Einbindung der Hygieneteams in diesen Bereich ist jedoch wenig untersucht.
Methode: Im Rahmen einer Umfrage unter Teilnehmenden der Freiburger Infektiologie- und Hygienekongresses 2024 wurden Einstellungen und Praktiken zum Thema Diagnostic Stewardship erfasst.
Ergebnisse: Die Mehrheit der 182 Teilnehmenden arbeitete in deutschen Krankenhäusern mit etablierten Hygienekommissionen (91,21%), Antibiotic Stewardship-Teams (43,41%) und Laborkommissionen (24,73%).
Bei der Sepsisdiagnostik werden meist mindestens zwei Blutkulturpaare entnommen, was den Leitlinien entspricht; 14,29% nutzen die „Six-Pack“-Regel (drei Paare), 28,57% nehmen alle Kulturen aus einer Punktionsstelle ab. Bei vielen klinischen Tests – mit Ausnahme von Stuhluntersuchungen und CRP – bewerteten weniger als 50% die Nutzung als „angemessen“, was auf Verbesserungsbedarf hinweist. IL-6 und Beta-D-Glucan werden selten verwendet.
Strategien wie Reflex-Tests und gesteuerte Antibiogramme werden nur gelegentlich verwendet und teils skeptisch betrachtet. Das Screening auf Methicillin resistente Staphylococcus aureus und Vancomycin resistant Enterokokken wurde von über 60% als „angemessen“ bewertet, beim Screening auf multiresistente Gram-negative Erreger von 50%. Bei den hygienespezifischen Fragen bewerten 32,4% eine Probenahmen von Oberflächen und 33,2% von den Händen des Personals als „zu wenig“.
Diskussion: Die Umfrage ist durch die subjektiven Einschätzungen der Teilnehmenden und eine heterogene Teilnehmerstruktur limitiert, zudem sind Subgruppenanalysen aufgrund geringer Fallzahlen nicht möglich. Die Ergebnisse zeigen Verbesserungspotential hinsichtlich der Einbindung der Hygieneteams beim Thema Diagnostic Stewardship und auch bei der Probenahme von Oberflächen und Händen.
Schlüsselwörter
Diagnostic Stewardship, Antibiotic Stewardship, Infektionskontrollteam
Introduction
In recent years, diagnostic stewardship has gained attention as part of antibiotic stewardship and infection control programs worldwide [1], [2], [3], [4], [5]. However, the involvement of infection control (IC) staff in these activities remains unclear and is not reported in the literature.
Method
To analyse the practice and attitudes regarding diagnostic stewardship among members of IC teams, we conducted a survey among visitors during the annual Freiburg conference of infection prevention and therapy 2024. Each participant agreed to take the survey and data-sheets (Attachment 1 [Att. 1]) were collected anonymously in drop-off-boxes.
Results
Table 1 [Tab. 1] shows the summary of the survey’s questions and the frequency of responses. Most of the 182 participants worked in German hospitals. Respondent’s institutions had an IC board, antibiotic stewardship teams, and a lab-commission specialized in diagnostic tests in 91.2%, 43.4%, and 24.7% respectively.
Table 1: Surveyed characteristics of participants and their evaluation of infection control and diagnostic stewardship guidelines and activities (n=182*)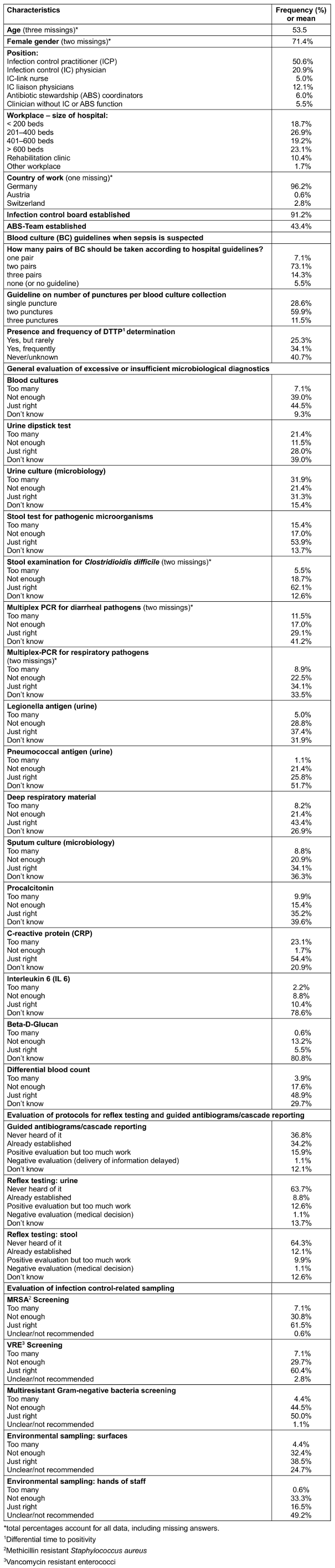
In most institutions a minimum of two pairs of blood cultures (BC) are taken for diagnosis of sepsis which is in accordance with current clinical guidelines. 14.3% have established the “six pack” rule (three pairs of BC) and 28.6% report collecting all blood cultures from a single puncture as recommended by emerging literature.
For most clinical test items with exception of stool testing and CRP, less than 50% of respondents felt that the utilization is “just right”, indicating relevant potential for improvement. IL 6 and Beta-D-Glucan are rarely utilized.
Diagnostic stewardship strategies like reflex testing and cascade reporting of resistance profiles are used only occasionally and sometimes met with scepticism.
Screening for MRSA and VRE was judged as “just right” by more than 60% of respondents, screening for multiresistant Gram-negative bacteria by 50%.
In the IC-related questions, 32.4% of respondents consider the amount of sampling to be insufficient regarding surface sampling while 33.2% believe the same for sampling from hands of staff.
Discussion
While the relatively high number of “unclear” answers in the specific test related questions can be explained by lack of involvement of the IC-Team members in clinical decision making, it also demonstrates the need for a more integrative approach between antibiotic stewardship and infection prevention.
The large number of respondents considering microbiological hand sampling as “not enough” came as a surprise considering much better educational tools for hand hygiene monitoring and motivation like real time fluorescent or dye-based visualization techniques; similarly, environmental surface sampling was often regarded as insufficient, although routine environmental sampling of surfaces is not recommended [6]. Van der Schoor et al. [7] conducted a web-based survey regarding environmental sampling in which most respondents were clinical microbiologists or infection prevention and control practitioners, and 57.3% were from either the Netherlands, the United Kingdom, or Ireland. Respondents had high self-reported knowledge, which was not consistent with their response to certain questions. There was no consensus on sample sites, neither within nor between countries [7]. Obviously, the same uncertainty exists in Germany.
Conclusion
The results indicate that German IC teams need more education and practical involvement in diagnostic stewardship activities not only in the context of antibiotic stewardship but also in their own field, given the high levels of uncertainty regarding environmental samples and hand hygiene related sampling.
Limitations
Our study is limited by the subjective nature of the answers and the large variety of professions. Overall, numbers in surveyed healthcare professions were too small for subgroup-analyses.
Notes
Authors’ ORCIDs
- Schulz-Stübner S: 0000-0001-5210-9364
Ethical approval
At a conference, participants agreed to participate in the voluntary anonymous survey.
Funding
This work was funded by institutional funds only.
Competing interests
The authors declare that they have no competing interests.
References
[1] Fabre V, Davis A, Diekema DJ, Granwehr B, Hayden MK, Lowe CF, Pfeiffer CD, Sick-Samuels AC, Sullivan KV, Van Schooneveld TC, Morgan DJ. Principles of diagnostic stewardship: A practical guide from the Society for Healthcare Epidemiology of America Diagnostic Stewardship Task Force. Infect Control Hosp Epidemiol. 2023 Feb;44(2):178-85. DOI: 10.1017/ice.2023.5[2] Claeys KC, Johnson MD. Leveraging diagnostic stewardship within antimicrobial stewardship programmes. Drugs Context. 2023 Feb 20;12:2022-9-5. DOI: 10.7573/dic.2022-9-5
[3] Schulz-Stübner S. Diagnostic Stewardship [Diagnostic Stewardship - The right test for the right patient with the right consequences]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2023 Sep;58(9):540-50. German. DOI: 10.1055/a-2154-1215
[4] Zakhour J, Haddad SF, Kerbage A, Wertheim H, Tattevin P, Voss A, Ünal S, Ouedraogo AS, Kanj SS; International Society of Antimicrobial Chemotherapy (ISAC) and the Alliance for the Prudent Use of Antibiotics (APUA). Diagnostic stewardship in infectious diseases: a continuum of antimicrobial stewardship in the fight against antimicrobial resistance. Int J Antimicrob Agents. 2023 Jul;62(1):106816. DOI: 10.1016/j.ijantimicag.2023.106816
[5] Jinks T, Subramaniam S, Bassetti M, Gales AC, Kullar R, Metersky ML, Poojary A, Seifert H, Warrier A, Flayhart D, Kelly T, Yu K, Altevogt BM, Townsend A, Marsh C, Willis C. Opportunities to Enhance Diagnostic Testing and Antimicrobial Stewardship: A Qualitative Multinational Survey of Healthcare Professionals. Infect Dis Ther. 2024 Jul;13(7):1621-37. DOI: 10.1007/s40121-024-00996-1
[6] Sehulster L, Chinn RY; CDC; HICPAC. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm Rep. 2003 Jun 6;52(RR-10):1-42.
[7] van der Schoor AS, Boyle M, Voor In 't Holt AF, Vos MC, Humphreys H; ESCMID Study Group for Nosocomial Infections. Environmental sampling of innate hospital surfaces: a survey of current practices and the need for guidelines. J Hosp Infect. 2022 Oct;128:92-5. DOI: 10.1016/j.jhin.2022.07.024
Attachments
| Attachment 1 | Survey items (Attachment1_dgkh000601.pdf, application/pdf, 163.87 KBytes) |

