The bopain.t questionnaire: evaluation of a current art therapy assessment tool
Susanne Maus-Hermes 1Gunnar Jähnichen 2
Sebastian Appelbaum 1
Constanze Schulze-Stampa 3
Thomas Ostermann 1
1 Department of Psychology and Psychotherapy, Witten/Herdecke University, Witten, Germany
2 Anesthesiology, Special Pain Therapy Delmenhorst, Palliative Medicine, Delmenhorst, Germany Nürtingen-Geislingen
3 Art Therapy, Nürtingen-Geislingen University of Applied Sciences, Nürtingen-Geislingen, Germany
Abstract
Chronic pain affects multiple areas of life and is closely linked to altered body perception. Given the high prevalence of chronic pain and the limited effectiveness of pharmacological monotherapies, multimodal pain treatment programs increasingly incorporate creative arts therapies. In this article, we introduce bopain.t, a new process-oriented approach within creative arts therapies designed for chronic pain treatment. The model integrates an art therapy intervention with an accompanying eight-item self-evaluation tool.
Based on two studies involving a clinical sample of chronic pain patients and a non-clinical sample of child and youth welfare workers, this article outlines the bopain.t approach, examines intervention effects, and presents first evidence for the validity of the bopain.t questionnaire. Principal component analysis conducted in the non-clinical sample resulted in a stable two-factor solution (Factor 1: Emotional experience with the creative process; Factor 2: Physical experience with the creative process), explaining 57.13% of the total variance. Seven items demonstrated consistent factor loadings, six of which showed strong loadings and conceptual interpretability. Importantly, the bopain.t scales were clearly distinguishable from conventional pain assessment instruments.
To further refine the instrument and relate its scales to established art therapy methods and embodiment constructs, additional validation studies are recommended.
1. Introduction
1.1 Chronic pain
Acute and chronic pain represent two distinct forms of pain [1], [2]. Acute pain is defined as a temporary warning signal from the body that is directly linked to tissue damage or impending injury, and it typically subsides once the underlying cause has healed [3]. In contrast, chronic pain affects multiple domains of daily life and often persists independently of ongoing tissue damage. A so-called pain memory may develop, giving the experience a momentum of its own [1], [2], [4]. Chronic pain constitutes a substantial personal and socio-economic burden [5], [6]; in Germany, approximately 27% of the population report persistent pain lasting longer than three months [6].
Clinically, chronic pain is commonly conceptualized along both somatic and psychological dimensions [7]. The somatic dimension includes reduced physical performance, generalization of pain, and discrepancies between clinical findings and subjective perception. The psychological dimension encompasses depressive symptoms, tendencies toward somatization, difficulties in coping, and social withdrawal [8].
1.2 Chronic pain and embodiment
Chronic pain affects patients’ sense of self, body perception, and emotional experience [9], [10], [11], [12], [13], [14], [15], [16]. The concept of embodiment, understood as the reciprocal interaction between body, mind, and environment [9], is particularly relevant in this context, as the relationship to one’s own body is often altered in chronic pain [10]. Research highlights the bidirectional influence between bodily processes and psychological states [11], [12], [13]. From a phenomenological perspective, chronic pain can further be understood as a disruption of the normally integrated body–mind relationship, in which bodily sensations become foregrounded and experienced as alien or intrusive [14]. For example, changes in posture have been shown to affect self-perception [13], [15], suggesting a meaningful relationship between mental states and the physical dimensions of pain [16].
1.2.1 Body perception of chronic pain patients
Chronic pain can lead to profound changes in the perception of one’s own body [17]. This may result in distortions in the perceived location of pain as well as altered sensations in adjacent body regions [18]. Neuroplastic changes in the central nervous system can affect both the sensory and motor cortex, leading to a blurred or diminished perception of tactile stimuli [19]. Spontaneous pain, heightened pain sensitivity (hyperalgesia), altered responses to mechanical stimuli, and restricted movement patterns are among the symptoms commonly associated with these changes [20].
From an embodiment perspective, the bidirectional interaction between body, mind, and environment becomes altered in chronic pain [9]. In healthy individuals, this relationship is characterized by a coherent integration of bodily and mental experience [10]. In contrast, under conditions of persistent pain, physical sensations become dominant and increasingly salient, drawing heightened attention to the bodily dimension of suffering [11]. Fuchs describes the experience of illness as a disruption of the unity between body and mind, leading to the “appearance” of physical symptoms as something felt separate or alien [14].
When pain persists or recurs for longer than three months [3], its protective warning function is no longer present. Instead, the underlying causes often remain unclear, while psychosocial factors become increasingly relevant [21]. Chronic pain is accompanied by changes in emotional experience, self-perception, social perception, posture, and social behavior [9]. Consequently, pain-related sensations vary depending on environmental conditions and subjective interpretations [22], as cognitive processes such as worry, attentional bias, and maladaptive problem-solving can contribute to the persistence and amplification of pain experience [22], [23]. Chronic pain therefore becomes a continuously present component of the patient’s lived experience.
1.3 Multimodal pain therapy
Because isolated pharmacological treatment is often insufficient [24], multimodal pain therapy programs (MMPTs) integrate medical, psychological, physical, and educational components [25], [26]. Psychological support plays a central role within these programs [26], [27], [28], [29], while complementary treatments, such as physiotherapy, relaxation techniques, mindfulness-based approaches, and creative arts therapies, contribute to improved pain management [30], [31]. MMPTs have been shown to enhance quality of life and support return-to-work outcomes [32], [33], while systematic reviews emphasize the heterogeneity of reported outcomes and the need for more differentiated, process-oriented assessment instruments in multimodal pain therapy [34]. Typical treatment duration ranges from two to four weeks and includes approximately 20 therapeutic sessions [25], [26]. Group-based interventions are considered advantageous due to their supportive dynamics and their potential to reduce the total number of treatment hours required [31], [35], [36].
1.4 Chronic pain and creative arts therapies
Chronic pain and creative arts therapies
Increasing evidence highlights the relevance of creative arts therapies in the treatment of chronic pain. Many approaches follow holistic principles that integrate cognitive, emotional, and sensory dimensions and aim to address both physical and psychological aspects of pain experience [37], [38], [39]. These findings indicate that creative and expressive interventions can be meaningfully incorporated into chronic pain care.
In addition to visual art-based approaches, body-based creative practices further demonstrate therapeutic potential. For example, dance and dance movement therapy interventions have been associated with improvements in body image, emotional well-being, and functional ability among individuals with fibromyalgia [40], [41]. Randomized controlled trials further suggest that structured dance interventions can significantly reduce pain and improve functional capacity and emotional well-being in this population, underscoring the importance of embodied creative expression in somatic perception and therapeutic change [41].
A new contribution to this field is the bopain.t model developed by our research group. It integrates physical, emotional, and creative dimensions and includes both a structured intervention and an eight-item self-assessment tool. Based on two studies, this article describes the bopain.t approach, evaluates the effects of the intervention, and presents initial findings on the validity of the bopain.t questionnaire.
2. Materials and methods
2.1 bopain.t intervention and questionnaire
2.1.1 bopain.t intervention
The intervention is based on a painting technique in which participants, standing upright, paint without a predefined motif for two minutes using eight colors and eight brushes. The process involves both large and small gestural movements, and the paint may be applied freely, through lines, strokes, or drops. The bopain.t intervention was therefore developed as a body-oriented, process-based method for individuals with chronic pain.
The intervention focuses not only on bodily experience but also on the dynamic perception of posture, movement, and emerging sensations. Its development was informed by artistic methods such as mess painting and the Creativity Mobilization Technique (CMT) [42], [43], which facilitate embodied, non-verbal forms of expression. These approaches enable the articulation of personal pain experiences, reactivated memories, and previously unexpressed emotions [44].
Contemporary perspectives emphasize complex interactions between neuroplastic processes, emotional experience, and implicit memory systems [45]. Building on these theoretical foundations, the bopain.t intervention was manualized and subsequently tested in an exploratory pilot study [46]. A central aspect of the method is the patient’s subjective experience during the art therapy process, particularly the perception of bodily sensations and emotional states.
2.1.2 bopain.t questionnaire
Because relatively little research has been conducted on the effectiveness or influencing factors of art therapy methods, only a limited number of standardized questionnaires are available to assess art therapy experiences. In recent years, several instruments have been developed, including the questionnaire on the experience of the art therapy group in psychosomatic medicine from the patient’s perspective (Fragebogen zum Erleben der Kunsttherapiegruppe aus Patientensicht, FEKTP) [47], the art therapy questionnaire (Fragebogen zur Kunsttherapie, FB-KT) [48], and the Self-Expression and Emotion Regulation in Art Therapy Scale (SERATS) [49]. These instruments allow for a systematic assessment of art therapy processes and outcomes.
A central focus of the FEKTP lies in evaluating the interaction between client and therapist, as well as the client’s perspective in both individual and group settings [47]. The FB-KT assesses process-related dimensions linked to individual needs for action and experience, including aspects relevant to pain perception that may be addressed through art therapy [48]. SERATS specifically targets processes of self-expression and emotion regulation within art therapy interventions [49].
In addition to examining the applicability of the bopain.t method within an inpatient multimodal pain therapy setting, there was a need to develop a complementary short and concise questionnaire capable of capturing individual experiences during art therapy sessions. This included perceptions related to relaxation and concentration, pain and bodily tension, as well as subjective emotional states.
Experiences gained from earlier applications of art therapy questionnaires [47], [48], together with conceptual and methodological insights from the exploratory pilot study underlying the development of the bopain.t intervention [46], served as the foundation for designing the bopain.t questionnaire. Its aim is to systematically capture individual, process-related experiences during the bopain.t art therapy procedure, with a particular focus on associated bodily sensations. The questionnaire consists of the following eight items (Table 1 [Tab. 1]).
Tablw 1: bopain.t questionnaire items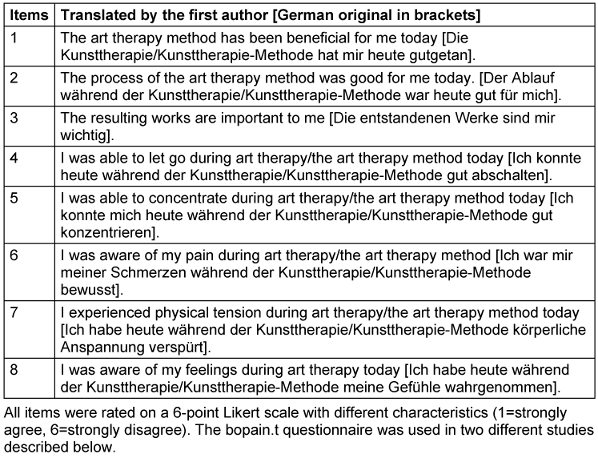
2.2 Study 1: chronic pain patients
In an exploratory observational pilot study with six measurement points, the bopain.t method was tested within a multimodal pain therapy (MMPT) program to assess the effects of the art therapy intervention on chronic pain patients during their inpatient stay.
2.2.1 Sample of study 1
The study was conducted with 20 adult patients aged 18 to 80 who suffered from chronic pain and were receiving inpatient multimodal pain therapy. All participants provided informed consent to take part in the study. One patient was excluded from the dataset due to incomplete data.
The average age of the remaining participants was 54.3 years, with a median age of 54.16 years. The youngest participant was 31 years old and the oldest 81, resulting in an age range of 50 years. On average, participants had been experiencing chronic pain for 10.9 years. Details are given in Tab. S1 in Attachment 1 [Att. 1].
The reported pain conditions included spinal pain, hip and lower leg pain, shoulder and thigh pain, medication-induced pain, headaches, and complex regional pain syndrome (CRPS). All patients confirmed that they had no previous experience with art therapy.
2.2.2 Setting
The MMPT at Josef-Hospital Delmenhorst, Germany, comprised a three-week inpatient treatment program in which patients received interdisciplinary care. The program included pharmacological pain management and orthopedic treatments, supplemented by various activating therapeutic modalities such as physiotherapy, biofeedback, occupational therapy, relaxation techniques, and music therapy. Psychotherapeutic and psychological treatments, offered four times per week, also formed an essential component of the program.
Multimodal pain therapy was predominantly delivered in group settings. For the duration of the study “bopain.t – an art therapy intervention for chronic pain patients: An exploratory pilot study in MMST”, the standard treatment program was expanded to include an additional art therapy module consisting of six interventions (two per week) of body-oriented painting (see Attachment 2 [Att. 2]) after which the bopain.t questionnaire was administered. Details are given in [46].
2.2.3 Instruments
In addition to the bopain.t questionnaire, socio-demographic questions were administered to capture participants’ profiles, including age, gender, duration of the chronic pain condition, and prior experience with art therapy, in accordance with international standards for reporting observational studies (STROBE) [50] and pain assessment in clinical research (IMMPACT) [51]. Pain intensity was assessed using a Visual Analogue Scale (VAS) [52], which was recorded at the beginning and at the end of the inpatient stay to quantify changes in perceived pain intensity.
2.2.4 Ethical considerations
Before the start of the studies, all participants were informed verbally and in writing about the study aims, the voluntary nature of participation, the handling of confidential data, the procedures for pseudonymization, and the time required for participation. Written informed consent was obtained from all participants. Consent could be withdrawn at any time without providing reasons and without negative consequences.
A discontinuation of the study would only have been considered if several participants had exhibited strong emotional or psychological reactions. Since emotional stimulation was an integral part of the therapeutic concept, discontinuation would have been initiated only in cases of particularly severe reactions.
The Ethics Committee for Art Therapies at Nürtingen/Geislingen University of Applied Sciences approved the study and all instruments used (positive vote dated 22 December 2017).
2.3. Study 2: employees in child and youth welfare services
In study two, the potential of art therapy methods as an instrument for systemic coaching for employees of child and youth welfare services was examined within a randomized cross-over study design. During the intervention phase, participants completed the bopain.t questionnaire at five measurement points, which served as the primary data source for the present evaluation.
2.3.1 Sample of study 2
Thirty-four German child and youth welfare workers participated in this study, most of whom were employed at the Duisburg Youth Welfare Office (n=29). In addition, a small external group (n=5) was included; although these participants did not share a common employer, they worked within similar professional contexts.
The average age of the participants was 38.5 years, with a median of 39 years and a modal age of 42 years (SD=10.78). The age range extended from 24 to 62 years.
Regarding educational background, 21 participants (61.8%) held a high school diploma, 11 (32.4%) had a vocational qualification, and two (5.9%) had completed secondary school. Five participants (14.7%) reported vocational training as their highest educational attainment, 18 (52.9%) held a bachelor’s degree, and ten (29.4%) reported a master’s degree or diploma.
Three main areas of professional activity were represented in the sample: child and youth welfare offices (three participants, 8.8%), youth welfare offices (22 participants, 64.7%), and kindergartens, schools, or after-school care facilities (nine participants, 26.5%). Details are given in Tab. S1 in Attachment 1 [Att. 1].
2.3.2 Setting
All participants received instruction in selected art therapy methods, including mandala drawing, free painting (see Attachment 2 [Att. 2]), and the bopain.t intervention. At time points A, C, and E, the art therapy sessions were conducted using analogue materials, such as paper and drawing utensils. At time points B and D, digital media were used instead, including a tablet and a digital drawing pen. All methods were embedded within a systemic coaching framework.
2.3.3 Instruments
As part of the preliminary assessment, socio-demographic data were collected across twelve categories using a standardized questionnaire, in line with international recommendations for reporting observational studies (STROBE) [50]. The survey captured the following characteristics: age, gender, educational background, professional field and function, length of service, working hours, workload, physical and psychological symptoms, and prior experience with art therapy or systemic coaching. Pain intensity was assessed using a Visual Analogue Scale (VAS) [52].
2.3.4 Ethical considerations
Individuals were eligible for inclusion if they were professionally active in the field of child and youth welfare, had obtained employer approval, were at least 18 years old, possessed unrestricted communication skills, and provided written informed consent. Prior to participation, all individuals received verbal and written information regarding the voluntary nature of the study, the handling of confidential data, the procedures for pseudonymization, and the expected time commitment. Written informed consent was obtained from all participants. They were informed that consent could be withdrawn at any time without providing reasons and without negative consequences, aside from the deletion of their data from the dataset.
The study “Art therapy methods as an instrument for systemic coaching for employees in youth welfare” was approved by the Ethics Committee of the University of Witten/Herdecke on 8 November 2023 (S-98/2022).
2.4 Statistical analysis
Due to the larger sample size, study 2 served as the primary data source for determining the structural relationships between the bopain.t items. Based on this sample, a principal component analysis (PCA) was conducted. One participant was excluded due to incomplete bopain.t data, resulting in a final sample of 33 participants for the PCA.
Although the sample size was acceptable for a conventional PCA of an eight-item instrument, a bootstrap procedure was applied to obtain a more robust empirical basis. Following the recommendations of Zientek and Thompson [53], sampling with replacement was performed 1,000 times in a two-step procedure: in the first step, one participant was randomly selected; in the second step, one measurement value from this individual’s five measurement points was drawn. This resulted in 1,000 resampled datasets, each containing 33 bopain.t values.
A PCA was performed on each bootstrap sample to identify structural relationships between the items. Eigenvalues and factor loadings were extracted from each analysis and evaluated using median and interquartile range statistics [53]. In this way, empirical estimates of eigenvalues and factor loadings were generated. The Kaiser-Gutman criterion (Eigenvalue >1) and Horn’s parallel analysis [54] were used to determine the number of factors. For Horn’s parallel analysis, 1,000 normally distributed random datasets were created and compared using their mean eigenvalues and the upper 95% percentile, as described by O’Connor [54].
Correlations between VAS pain and the emerging bopain.t scales were analyzed using Pearson’s correlation coefficient. The progression of the bopain.t scales across measurement points was visualized graphically. Items of the scales have not been reversed.
Unless otherwise stated, a p-value smaller than or equal to .05 was considered statistically significant. All analyses were conducted using SPSS (Version 29).
3. Results
3.1 Principal Component Analysis (PCA)
Based on the sample from study 2, the principal component analysis (PCA) yielded the factor loadings shown in Table 2 [Tab. 2].
Table 2: Factor loadings of the bopain.t items (factor loadings >0.40 are presented in bold)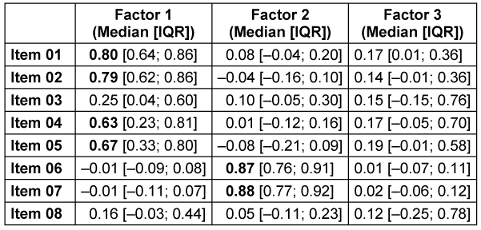
The first factor was formed by items 1 (“The art therapy method has been beneficial for me today”), 2 (“The process during the art therapy method was good for me today”), 4 (“I was able to switch off well today during the art therapy method”), and 5 (“I was able to concentrate today during the art therapy method”). All these items loaded on a common factor. Their median factor loadings exceeded 0.60, which, according to the recommendations in [55], is sufficient to indicate a clear association with the factor. This factor was termed “Emotional experiences with the creative process.”
The second factor, termed “Physical experience with the creative process” comprised items 6 (“I was aware of my pain during the art therapy method”) and 7 (“I experienced physical tension during the art therapy method today”). Both items showed factor loadings of similar magnitude (0.87 and 0.88).
Items 3 (“The resulting works are important to me”) and 8 (“I aware of my feelings today during the art therapy method”) did not exhibit sufficiently strong or consistent loadings to justify the extraction of a third factor. Consequently, they were not included in the construction of the bopain.t scales. Figure 1[Fig. 1] presents the full bootstrap-derived sampling distributions of the factor loadings for Factors 1 and 2.
Figure 1: Empirically estimated sampling distributions of the factor loadings for Factor 1 (left) and Factor 2 (right). The distributions are visualized using box plots, which display the median (black line), the interquartile range (grey box), and statistical outliers (circles).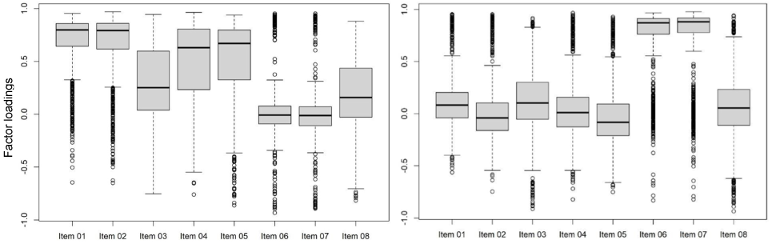
The distribution of eigenvalues across the 1,000 bootstrap samples is presented in Figure 2 [Fig. 2]. The first factor showed a median eigenvalue of 2.76 (IQR: [2.55; 3.00]), clearly exceeding the critical value of 1 and accounting for 34.5% of the total variance. The second factor also met the Kaiser-Gutman criterion, with a median eigenvalue of 1.81 (IQR: [1.68; 1.93]), explaining 22.6% of the variance.
Figure 2: Empirically estimated eigenvalues for the factors of the PCA. The distributions are visualized using box plots displaying the median (black line), the interquartile range (grey box), and statistical outliers (circles). The cut-off value for factor retention according to the Kaiser–Gutman criterion (Eigenvalue >1) is indicated by the blue line.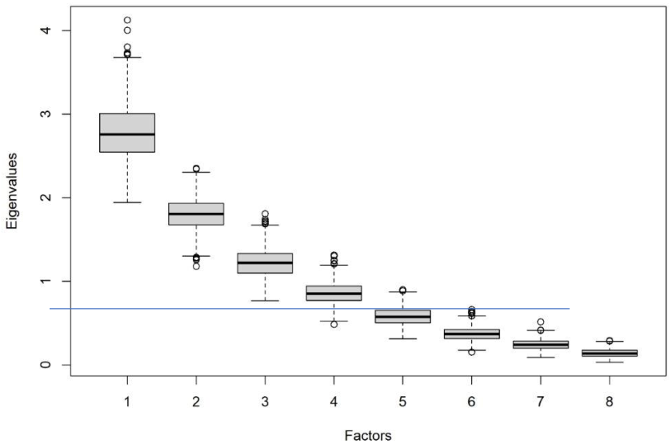
Factor 3, associated with Item 8 (“I aware of my feelings today during the art therapy method”), exhibited an eigenvalue slightly above 1 (1.22, IQR: [1.10; 1.33]); however, this value was only marginally higher than the threshold, indicating insufficient strength to justify the extraction of an additional factor.
In Figure 3 [Fig. 3], the first two factors lie clearly above the upper bound of the 95% confidence interval (green line), whereas Factor 3, with an Eigenvalue of 1.15, only marginally exceeds the Eigenvalue criteria, which confirms the analyses from Figure 2 [Fig. 2]. Taking into account this still unclear data situation, it appears that a separate single-item factor is not justified at the moment. Therefore, and because it was a single item, Factor 3 was not retained for further analysis.
Figure 3: Scree plot of the eigenvalues from the original dataset (“raw data”; blue line) compared with the mean Eigenvalues derived from 1,000 normally distributed random datasets (“means”; red line). The turquoise line (“percntyl”) represents the upper bound of the 95% confidence interval.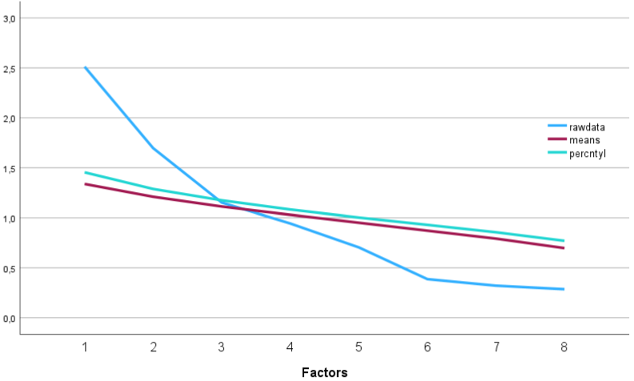
3.2 Correlations with VAS Pain
In the second study, correlations between the bopain.t factors and VAS pain were assessed at each measurement point. The results of this exploratory analysis are presented in Table 3 [Tab. 3].
Table 3: Correlations (r, Pearson) between the bopain.t factors and VAS pain at sessions A, B, C, D, and E (see text for further explanation). Significant correlations are marked with an asterisk (*).
The correlations between the bopain.t factors and VAS pain levels showed substantial variability across the different measurement points. At time points A, C, and E, the art therapy intervention was conducted with analogue materials (paper and drawing utensils), whereas at time points B and D digital media (tablet and digital pen) were used. This pattern suggests that Factor 1, “Emotional experience with the creative process”, correlates more strongly with pain perception in conditions shaped by the respective creative medium.
Factor 2, “Physical experience with the creative process”, showed moderate to high negative correlations with VAS pain at time points A and B, but no meaningful correlations at time points C, D, and E.
In a further validation step, based on the data from study 1, the development of the bopain.t subscales over the course of the multimodal pain treatment is illustrated in Figure 4 [Fig. 4].
Figure 4: Development of Factor 1, “Emotional experience with the creative process” and Factor 2, “Physical experience with the creative process” over the course of time compared to the VAS-Pain scale. Error bars denote the 95% Confidence intervals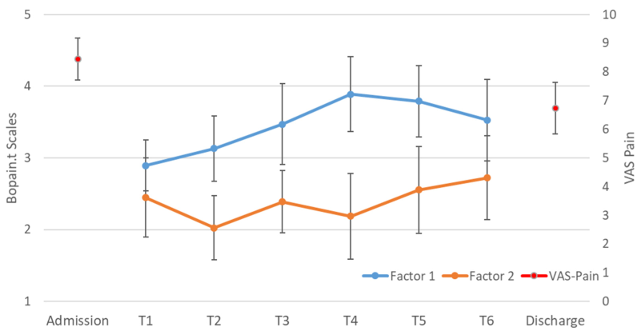
Figure 4 [Fig. 4] shows that patients’ pain perception (VAS pain) decreased significantly over the course of the multimodal pain therapy, from 8.45±1.21 at admission to 6.73±1.49 at discharge (t=4.503, df=10; p=0.001).
Factor 2, “Physical experience with the creative process” (orange line in Figure 4 [Fig. 4]), remained relatively stable over time, which was confirmed by a repeated-measures ANOVA with Greenhouse-Geisser correction (F=1.64; p=0.184).
In contrast, Factor 1, “Emotional experience with the creative process” (blue line in Figure 4 [Fig. 4]), showed an increase from T1 to T4 followed by a slight decline. This pattern was statistically significant (repeated-measures ANOVA with Greenhouse-Geisser correction: F=4.65; p=0.002).
4. Discussion
In our study, factor analysis yielded a stable and convergent two-factor solution (Factor 1: Emotional experience with the creative process; Factor 2: Physical experience with the creative process), identifying bopain.t as a valid instrument for assessing process-related experiences in art therapy.
While temporal changes in the experience of the art therapy process were clearly observable, no direct association emerged between the bopain.t scales and current pain intensity. This suggests that the bopain.t scales do not primarily capture pain perception but instead reflect aspects of body awareness and engagement during the art therapy process. However, this interpretation must be treated with caution, as mindfulness-related processes, strongly connected to attentional and interoceptive mechanisms, are also known to influence pain processing and pain perception [56], [57]. Moreover, the fact that VAS pain and bopain.t ratings were not collected at identical time points represents an additional source of potential bias.
The results of the correlation analysis for Factor 1 (“Emotional experience with the creative process”) suggest that aesthetic engagement may facilitate a connection to bodily experience and physical perception. In contrast, the pattern observed for Factor 2 (“Physical experience with the creative process”) indicate that the physical component of the art therapy intervention may be less pronounced in this sample, likely because the participants of study 2 were not chronic pain patients.
Recent models of art therapy additionally emphasize emotion processing as a central mechanism of therapeutic change, particularly regarding the regulation, expression, and integration of affective experiences during the therapeutic process [58] .
Given these aims, systematically recording participants’ subjective experiences becomes particularly important. Although several questionnaires have been developed to assess patients’ experiences with art therapy in healthcare settings [47], [48], the bopain.t questionnaire was specifically designed to illuminate both conscious and unconscious perceptions arising during the art therapy process, distinguishing it from existing instruments. Its primary purpose is to capture individual experiential qualities within the session, including aspects of therapeutic interaction and relationship quality that are central to art therapy processes [59].
Such tools, which support both documentation and self-reflection, have gained increasing relevance in art therapy research [60], [61]. Recent scientific discussions emphasize the importance of incorporating the client’s perspective when examining the potential effects of art therapy methods [59], [60], [62]. From a clinical standpoint, growing attention is being directed toward psychological, physical, and emotional dimensions of therapeutic experience [63].
5. Limitations
From a methodological perspective, the sample size for a validation study was relatively small. Nevertheless, previous research has shown that exploratory factor analytic approaches can yield reliable results even with N<50 when the data are well-conditioned [64]. In such cases, resampling procedures are recommended. Therefore, we applied a bootstrapping approach, which has been successfully used in principal component analysis to obtain more stable and interpretable parameter estimates [65].
Despite the promising psychometric properties demonstrated in this study, the current results are not yet sufficient to recommend the bopain.t questionnaire as a standalone instrument in scientific practice. Further validation is required, ideally including comparisons with established instruments in related domains such as mindfulness and embodiment, to sharpen the instrument’s conceptual profile. This applies above all to the factor structure. Here, based on corresponding indications from the research literature [66], we decided against a third single-item factor. A future research approach could consist of expanding this factor into a valid dimension by adding further suitable items. It also remains to be seen to what extent the designation of the first factor as “Emotional experience with the creative process” will remain stable after corresponding studies have been conducted. Such studies could also show that there is a stronger connection to “Cognitive experiences with art therapy” and that a renaming would therefore be appropriate.
Future studies should also examine whether the questionnaire is applicable across different art therapy interventions. Finally, the bopain.t questionnaire is currently available only in German, a validation of an English version does not yet exist.
6. Conclusions
In sum, the bopain.t questionnaire represents a promising instrument for capturing individual perceptions of art therapy processes. In addition, it highlights both conscious and unconscious aspects of self-awareness. Although the instrument was originally developed for use within the bopain.t art therapy procedure, it may also be applicable in other art therapy contexts. Owing to its compact format, it is quick and easy to administer and can be seamlessly combined with other assessment tools. Nevertheless, additional research is needed to establish its reliability and validity more robustly
Notes
Competing interests
The authors declare that they have no competing interests.
Data availability
Information regarding the intervention and additional data can be obtained from the corresponding author upon request.
Ethics statement
The studies were approved by the respective ethics committees (Ethics Committee for Art Therapies at the Nürtingen/Geislingen University of Applied Sciences, 22.12.2017: Study 1) and University of Witten/Herdecke, S-98/2022, 8.11.2023: Study 2) and were conducted in accordance with the Declaration of Helsinki. All participants provided informed consent.
References
[1] Jähnig W, Baron R. Pathophysiologie des Schmerzes. In: Fischer L, Peuker ET, Hrsg. Lehrbuch Integrative Schmerztherapie. Stuttgart: Haug Verlag; 2011. S. 35–67.[2] Nobis HG, Rolke R. Akuter und chronischer Schmerz. In: Nobis HG, Rolke R, Graf-Baumann T, Förderreuther S, Hüppe M, Sommer C, Hrsg. Schmerz – eine Herausforderung: Ein Ratgeber für Betroffene und Angehörige. Berlin: Springer; 2020. S. 6–7.
[3] Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. DOI: 10.1097/j.pain.0000000000000160
[4] Kleinböhl D, Baus D, Hornberger U, Hölzl R. Schmerzgedächtnis und Sensibilisierung. Psychoneuro. 2005;31(2):84–91. DOI: 10.1055/s-2005-865115
[5] Kieselbach K, Schittenwolf M, Bozzaro C. Versorgung chronischer Schmerzen: Wirklichkeit und Anspruch. Schmerz. 2016;30(4):351–357. DOI: 10.1007/s00482-016-0137-2
[6] Kaiser U, Nagel B, Petzke F, Pfingsten M, Gärtner A, Isenberg T, et al. Vermeidung chronischer Schmerzen in der deutschen Gesundheitsversorgung. Schmerz. 2021;35:45–52. DOI: 10.1007/s00482-020-00527-0
[7] Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. DOI: 10.1037/0033-2909.133.4.581
[8] Arnold B, Brinkschmidt T, Casser HR, Gralow I, Irnich D, Klimczyk K, et al. Multimodale Schmerztherapie: Konzepte und Indikation. Schmerz. 2009;23(2):112–120. DOI: 10.1007/s00482-008-0741-x
[9] Fuchs T. Ecology of the brain: The phenomenology and biology of the embodied mind. Oxford: Oxford University Press; 2018.
[10] Gallagher S. How the body shapes the mind. Oxford: Oxford University Press; 2005.
[11] Fuchs T. The phenomenology of body memory. In: Koch SC, Fuchs T, Summa M, Müller C, Hrsg. Body memory, metaphor and movement. Amsterdam: John Benjamins; 2012. S. 9–22.
[12] Kuehn A, Holle D, Bingel U. Körper, Schmerz und Bewusstsein: Wie Embodiment-Ansätze die Schmerztherapie verändern. Schmerz. 2020;34(4):339–346. DOI: 10.1007/s00482-020-00437-7
[13] Koch SC. Embodiment: Der Einfluss von Eigenbewegung auf Affekt, Einstellung und Kognition. Berlin: Logos Verlag; 2013.
[14] Fuchs T. Ökologie des Gehirns: Eine systemische Sichtweise für Psychiatrie und Psychotherapie. Nervenarzt. 2005;76(1):1–10. DOI: 10.1007/s00115-004-1816-2
[15] de Vignemont F. Embodiment, ownership and disownership. Conscious Cogn. 2011;20(1):82–93. DOI: 10.1016/j.concog.2010.09.004
[16] Mehling WE, Price C, Daubenmier JJ, Acree M, Bartmess E, Stewart A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS One. 2012;7(11):e48230. DOI: 10.1371/journal.pone.0048230
[17] Lauche R, Cramer H, Haller H, Musial F, Langhorst J, Dobos GJ, et al. My back has shrunk: The influence of traditional cupping on body image in patients with chronic non-specific neck pain. Forsch Komplementmed. 2012;19(2):68–74. DOI: 10.1159/000337688
[18] Moseley GL, Herbert RD, Parsons T, Lucas S, Van Hilten JJ, Marinus J. Intense pain soon after wrist fracture strongly predicts who will develop complex regional pain syndrome: Prospective cohort study. J Pain. 2014;15(1):16–23. DOI: 10.1016/j.jpain.2013.08.009
[19] Wand BM, Tulloch VM, George PJ, Smith AJ, Goucke R, O’Connell NE, Moseley GL. Seeing it helps: Movement-related back pain is reduced by visualization of the back during movement. Clin J Pain. 2012;28(7):602–608. DOI: 10.1097/AJP.0b013e31823d480c
[20] Brunner F. Komplexes regionales Schmerzsyndrom. Z Rheumatol. 2017;76(4):335–347. DOI: 10.1007/s00393-017-0299-z
[21] Craig KD. The social communication model of pain. Can Psychol. 2009;50(1):22–32. DOI: 10.1037/a0014772
[22] Eccleston C, Crombez G. Worry and chronic pain: A misdirected problem-solving model. Pain. 2007;132(3):233–236. DOI: 10.1016/j.pain.2007.09.014
[23] Becker A, Straßner C. S1-Leitlinie Chronischer Nicht Tumorbedingter Schmerz. Berlin: AWMF; 2023. Available from: https://register.awmf.org/assets/guidelines/053-036l_S1_Chronischer_Schmerz_2023-12.pdf
[24] Kieselbach K, Koesling D, Wabel T, Frede U, Bozzaro C. Chronischer Schmerz als existenzielle Herausforderung. Schmerz. 2023;37(2):116–122. DOI: 10.1007/s00482-022-00632-2
[25] Arnold B, Brinkschmidt T, Casser HR, Diezemann A, Gralow I, Irnich D, et al. Multimodale Schmerztherapie für die Behandlung chronischer Schmerzsyndrome. Schmerz. 2014;28(5):459–472. DOI: 10.1007/s00482-014-1471-x
[26] Deckert S, Kaiser U, Kopkow C, Trautmann F, Sabatowski R, Schmitt J. A systematic review of the outcomes reported in multimodal pain therapy for chronic pain. Eur J Pain. 2016;20(1):51–63. DOI: 10.1002/ejp.721
[27] Nijs J, Malfliet A, Roose E, Lahousse A, Van Bogaert W, Johansson E, et al. Personalized multimodal lifestyle intervention as the best-evidenced treatment for chronic pain. J Clin Med. 2024;13(3):644. DOI: 10.3390/jcm13030644
[28] Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM). Operationen- und Prozedurenschlüssel (OPS). Bonn: BfArM; 2025.
[29] Koch U, Mehnert A, Strauss B. Psychologische Interventionen bei chronisch körperlich kranken Patienten mit psychischer Komorbidität. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2011;54(1):29–36. DOI: 10.1007/s00103-010-1186-9
[30] van Tulder MW, Koes B, Malmivaara A. Outcome of non-invasive treatment modalities on back pain: An evidence-based review. Eur Spine J. 2006;15(Suppl 1):S64–S81. DOI: 10.1007/s00586-005-1048-6
[31] Raudenská J, Šteinerová V, Vodičková Š, Raudenský M, Fulková M, Urits I, et al. Arts therapy and its implications in chronic pain management: A narrative review. Pain Ther. 2023;12(6):1309–1337. DOI: 10.1007/s40122-023-00542-w
[32] Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P, et al. Diagnosis and treatment of low back pain. Ann Intern Med. 2007;147(7):478–491. DOI: 10.7326/0003-4819-147-7-200710020-00006
[33] Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, van Tulder MW. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst Rev. 2014;9:CD000963. DOI: 10.1002/14651858.CD000963.pub3
[34] Shi Y, Wu W. Multimodal non-invasive non-pharmacological therapies for chronic pain: Mechanisms and progress. BMC Med. 2023;21(1):372. DOI: 10.1186/s12916-023-03076-2
[35] Strauß B, Burlingame GM, Rosendahl J. Neue Entwicklungen in der Gruppenpsychotherapieforschung – ein Update. Psychotherapeut. 2020;65(4):225–235. DOI: 10.1007/s00278-020-00430-0
[36] Schulze-Stampa C. Gruppendynamische Potenziale der Kunsttherapie. Neuroreha. 2022;14(2):69–73. DOI: 10.1055/a-1816-5546
[37] Kalmanti A, Batistaki C, Christodoulou C, Gerolouka-Kostopanagiotou G, Douzenis A, Michopoulos I. Hybrid arts-based CBT for chronic pain. Psychiatriki. 2022;33(3):187–199. DOI: 10.22365/jpsych.2022.064
[38] Barnett KS, Vasiu F. How the arts heal. Front Behav Neurosci. 2024;18:1422361. DOI: 10.3389/fnbeh.2024.1422361
[39] Haeyen S. Effects of art therapy. Arts Psychother. 2018;61:1–8. DOI: 10.1016/j.aip.2018.10.002
[40] Shim M, Johnson RB, Gasson S, Bradt J. Dance/movement therapy model. Eur J Integr Med. 2017;9:27–40. DOI: 10.1016/j.eujim.2016.10.005
[41] Baptista AS, Villela AL, Jones A, Natour J. Dance in fibromyalgia. Clin Exp Rheumatol. 2012;30(Suppl 74):S18–S23.
[42] Schottenloher G. Messpainting I. In: Baukus P, Thies J, Hrsg. Aktuelle Tendenzen in der Kunsttherapie. Stuttgart: Gustav Fischer; 1993. S. 37–52.
[43] Schottenloher G. Messpainting II. In: Schottenloher G, Schnell H, Hrsg. Wenn Worte fehlen, sprechen Bilder. München: Kösel; 1994. S. 58–85.
[44] Roth G. Bildung braucht Persönlichkeit. Stuttgart: Klett-Cotta; 2021.
[45] Schacter DL. Searching for memory. New York: Basic Books; 1996.
[46] Maus-Hermes S. bopain.t – eine kunsttherapeutische Intervention für chronische Schmerzpatienten [Masterarbeit]. Ottersberg: HKS Ottersberg; 2018.
[47] Ganter-Argast C, Teufel M, Sammet I, Tagay S, Zipfel S, Mander J. FEKTP-Fragebogen. Psychother Psychosom Med Psychol. 2019;69(7):283–292. DOI: 10.1055/a-0667-7827
[48] Scherdt C, Witz M, Grabbe Y, Gralow I. Art therapy questionnaire. Psychotherapeut. 2002;47(5):301–309. DOI: 10.1007/s00278-002-0241-x
[49] Haeyen S, van Hooren S, van der Veld WM, Hutschemaekers GJM. SERATS validation. Arts Psychother. 2015;45:106–112. DOI: 10.1016/j.aip.2015.07.002
[50] von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE statement. Lancet. 2007;370(9596):1453–1457. DOI: 10.1016/S0140-6736(07)61602-X
[51] Dworkin RH, Turk DC, Farrar JT, et al. IMMPACT recommendations. Pain. 2005;113(1–2):9–19. DOI: 10.1016/j.pain.2004.09.012
[52] Huskisson EC. Measurement of pain. Lancet. 1974;2(7889):1127–1131.
[53] Zientek LR, Thompson B. Bootstrap factor analysis. Behav Res Methods. 2007;39(2):318–325. DOI: 10.3758/BF03193163
[54] O’Connor BP. Parallel analysis programs. Behav Res Methods Instrum Comput. 2000;32(3):396–402. DOI: 10.3758/BF03200807
[55] Floyd FJ, Widaman KF. Factor analysis in clinical instruments. Psychol Assess. 1995;7(3):286–299. DOI: 10.1037/1040-3590.7.3.286
[56] Hölzel BK, Lazar SW, Gard T, Schuman-Olivier Z, Vago DR, Ott U. Mindfulness meditation. Perspect Psychol Sci. 2011;6(6):537–559.
[57] Ploesser M, Martin D. Mechanism of mindfulness for pain. J Integr Complement Med. 2024;30(12):1162–1178.
[58] Czamanski-Cohen J, Weihs KL. REPAT model. Front Psychol. 2023;14:1208901.
[59] Schulze C, Sinapius P, Kasper J. Entwicklung integrativer Behandlungskonzepte. Ottersberg: HKS; 2010.
[60] Rankanen M. Art therapy group experiences. Arts Psychother. 2016;50:101–110.
[61] Masuch J, Brons S, Habboub B, et al. Kunsttherapie Geriatrie. Psychotherapie. 2023;68(4):271–279.
[62] Betts DJ. Art therapy assessments. Arts Psychother. 2006;33(5):422–434.
[63] Huber A, Zimmermann J, Wessa M. Resilienz bei chronischem Stress. Verhaltenstherapie. 2022;32(1):33–44.
[64] de Winter JC, Dodou D, Wieringa PA. Small-sample factor analysis. Multivariate Behav Res. 2009;44(2):147–181.
[65] Babamoradi H, van den Berg F, Rinnan Å. Bootstrap PCA. Chemom Intell Lab Syst. 2013;120:97–105.
[66] Loo R. Single vs multiple-item scales. J Manag Psychol. 2002;17(1):68–75.

