[Deutsche Übersetzung und kulturelle Anpassung des Hearing Environments and Reflection on Quality of Life (HEAR-QL26) Fragebogens für Kinder im Alter von 7 bis 12 Jahren]
Vanessa Hoffmann 1Julia Hannah Quitmann 2
Manfred Hintermair 3
1 Hamburg University of Applied Sciences, Faculty of Health, Hamburg, Germany
2 Hamburg University of Applied Sciences, Faculty of Business and Social Sciences, Chair of Applied Developmental Psychology, Hamburg, Germany
3 Heidelberg University of Education, Heidelberg, Germany
Zusammenfassung
Zielsetzung: Diese Studie hatte zum Ziel, den Hearing Environments and Reflection on Quality of Life(HEAR-QL26)-Fragebogen für Kinder im Alter von 7 bis 12 Jahren mit Hörbeeinträchtigung ins Deutsche zu übersetzen und kulturell anzupassen. Ziel war es, die semantische, konzeptuelle und kulturelle Äquivalenz sicherzustellen und ein valides Instrument zur Erfassung der hörbezogenen Lebensqualität in dieser Population bereitzustellen.
Methode: Die Adaptation erfolgte nach internationalen Richtlinien zur kulturübergreifenden Übersetzung hörbezogener Erhebungsinstrumente. Der Prozess umfasste folgende Schritte: (1) Vorbereitung, (2) Vorwärtsübersetzung durch unabhängige Übersetzer, (3) Abgleich der Übersetzungen, (4) Rückübersetzung, (5) Überprüfung durch ein Expertengremium sowie (6) Feldtestung mittels kognitiver Interviews. Das Feedback aus den Interviews wurde genutzt, um den Fragebogen zu überarbeiten. Alle Änderungen wurden erneut rückübersetzt und durch das Expertengremium geprüft, bis ein Konsens erreicht war.
Ergebnisse: Der Prozess zeigte Herausforderungen bei der Erreichung einer vollständigen semantischen Äquivalenz, insbesondere bei Begriffen ohne direkte deutsche Entsprechung. In der ersten Testung mit zehn Kindern erwiesen sich mehrere Items als schwer verständlich, was zur Vereinfachung der Formulierungen, Zusammenführung redundanter Items und Entfernung komplexer Vergleichsfragen führte. Die überarbeitete Version wurde anschließend mit den ursprünglichen zehn und vier weiteren Kindern (n=14) getestet und bestätigte eine verbesserte Verständlichkeit und Angemessenheit. Die finale deutsche Version des HEAR-QL umfasst 25 Items in leicht verständlicher Sprache und weist eine starke konzeptuelle Übereinstimmung mit dem Originalinstrument auf.
Schlussfolgerungen: Die Studie verdeutlicht die Machbarkeit und die Herausforderungen bei der Adaptation eines komplexen pädiatrischen Lebensqualitätsfragebogens in eine andere Sprache und kulturellen Kontext. Obwohl die deutsche Version des HEAR-QL25 die konzeptuelle Treue zum Original weitgehend beibehält, konnten bestimmte semantische Nuancen nicht vollständig übertragen werden. Die kleine und homogene Stichprobe begrenzt zudem die Generalisierbarkeit der Ergebnisse. Trotz dieser Einschränkungen stellt die adaptierte Version ein vielversprechendes Instrument zur Erfassung der hörbezogenen Lebensqualität bei deutschsprachigen Kindern dar. Eine weiterführende Validierung in größeren und diverseren Stichproben wird empfohlen.
Schlüsselwörter
Lebensqualität, Kinder mit Hörverlust, kulturübergreifende Adaptation, deutsche Übersetzung, patientenberichtete Ergebnismaße (PROMs)
Introduction
Hearing loss in childhood can significantly interfere with speech and language development, cognitive functioning, and social-emotional growth, often resulting in long-term educational and psychosocial consequences [1], [2]. Early identification and rehabilitation have therefore become core components of pediatric audiological care. However, in recent years, there has been increasing recognition that clinical metrics such as audiograms or speech perception tests alone do not sufficiently capture the lived experiences of children with hearing loss. This has led to a broader emphasis on health-related quality of life (HRQoL) as a critical dimension in evaluating treatment outcomes [3], [4], [5], [6].
Patient-reported outcome measures (PROMs) offer a systematic way to assess how individuals perceive the impact of their condition on daily life. In pediatric populations, age-appropriate PROMs allow for the inclusion of children’s own perspectives, or—when necessary—the insights of caregivers. Such instruments support patient-centered care by integrating subjective well-being into clinical decision-making and by promoting shared understanding between professionals, patients, and families [7].
Generic quality of life instruments, while useful in broad health contexts, often lack the sensitivity to detect the specific effects of hearing loss on a child’s everyday experiences [8]. In contrast, condition-specific tools like the Hearing Environments and Reflection on Quality of Life (HEAR-QL26) questionnaire have been developed to address this gap. The HEAR-QL26 is a self-report instrument tailored for children aged 7 to 12 years, assessing the impact of hearing difficulties on school participation, peer interactions, 20 emotional well-being, and daily listening environments [9]. Its structure is specifically designed to reflect the cognitive and communicative abilities of school-aged children, making it suitable for capturing their subjective health perceptions.
To use such tools in non-English-speaking populations, a rigorous process of linguistic translation and cultural adaptation is required. This process ensures not only semantic equivalence but also conceptual and contextual appropriateness within the target language and culture. Best practices in this field advocate for a multistep approach including forward and backward translation, expert panel reviews, and cognitive testing with the target population [10]. This methodology helps ensure that the adapted version retains the validity and reliability of the original instrument.
The present study describes the German translation and cultural adaptation of the HEAR-QL26 questionnaire for children aged 7 to 12 years. This developmental stage is marked by increasing social and academic demands, making the ability to assess hearing-related quality of life particularly relevant. By providing a culturally and linguistically appropriate version of the HEAR-QL26, the study aims to support clinicians and researchers in evaluating outcomes from the perspective of affected children themselves, thereby contributing to more comprehensive, child-centered audiological care. By enabling clinicians to access children’s own perspectives on hearing-related challenges, this adaptation supports more nuanced, empathetic, and effective audiological care. In developing the present version, we adhered closely to the conceptual framework of the original English instrument; therefore, no modifications were made to the categories or items, and we do not engage here in a discussion of their conceptual validity.
The following sections outline the multistep methodology used to ensure linguistic and cultural fidelity in the German adaptation.
Methods and results
The translation and cultural adaptation of the HEAR-QL26 questionnaire into German was carried out in accordance with established international guidelines for the linguistic transfer of hearing-related instruments [10]. The workflow included forward translation, reconciliation, back translation, expert panel review, cognitive debriefing with children, and final proofreading. The adaptation team included a diverse group of contributors with complementary areas of expertise. These included certified translators, clinical experts, academic researchers, and end users with hearing loss. Throughout the process, the coordination was managed by the lead translator, who, together with a second team member, held academic qualifications in hearing rehabilitation and special education. Both were native speakers of German, professionally trained as speech-language therapists, and fluent in English. The original developer of the source-language questionnaire contributed domain-specific expertise and offered guidance to ensure fidelity to the original instrument’s conceptual framework. A bilingual linguist, who had lived and worked in both German- and English-speaking environments and had expertise in Deaf studies and sign language, was consulted during the review stages to evaluate semantic equivalence and cultural sensitivity. In addition to expert review, native-speaking children with hearing loss were actively involved in the process. Their input was collected through individual interviews to assess whether the translated items were meaningful, understandable, and relevant to daily experiences. Their feedback informed several refinements to the language used in the German version, helping ensure that it was both accessible and appropriate for the target population of school-aged children with hearing loss.
Step 1: Preparation
As part of the preparatory phase, the project lead contacted the original developer of the HEAR-QL to confirm the absence of a documented German version and to obtain written consent for adaptation. Throughout the translation, he was consulted whenever questions arose concerning the methodology or the original questionnaire content. A structured documentation template, adapted from Hall et al. (2018) [10], was used to record each step of the translation and cultural adaptation process, including translator roles, review stages, and feedback integration. Potential differences between the English-speaking source population and the German-speaking target group were carefully examined by two authors. A comparative analysis of literacy levels, age distribution, and questionnaire delivery methods between English-speaking and German-speaking populations revealed no substantive differences, supporting the retention of the original language complexity and format. Therefore, it was unnecessary to alter the language complexity or the format of administration.
Step 2: Forward translation
In the second phase, the questionnaire was translated from the original English into German. Initially, both the translation lead and a professional translator from a language service independently rendered the items into German. The professional translator was briefed about the questionnaire’s objectives and its intended audience, as well as the fact that this translation was part of a larger, multi-step adaptation process. Both translations were completed independently, informed by the translators’ familiarity with health-related terminology and the questionnaire’s objectives. Following the independent translations, a third party—an impartial team member—reviewed both versions, identifying discrepancies and providing justification for preferred wording choices. The reviewer evaluated both versions for semantic accuracy, age-appropriate language, and alignment with the original intent. While most items showed minor lexical differences, five required more substantial revision due to idiomatic expressions or culturally specific references. These were resolved through consensus discussions. The rating scale, the categories and one item out of 26 were identical across translations, while for all 26 items, the reviewer selected the preferred version. For example, the item had two German translations: “Do you have a hard time hearing your friends at recess?” – “Fällt es dir schwer, deine Freunde in der Pause zu hören?” and “Fällt es dir schwer, deine Freunde in der Pause zu verstehen?”. The reviewer favored “verstehen” (understanding the content) as it better reflected the original meaning than “hearing” (just listening without interpreting).
Step 3: Back translation
The preliminary German version of the questionnaire was then translated back into English by a separate professional translator. The purpose of this back translation was to verify that the translated version maintained the same meaning as the original questionnaire. Any discrepancies between the back-translated items and the original were identified and addressed. The translation lead carefully compared the back-translated text with the original questionnaire, examining all items for differences in wording or sentence structure. Sections that did not align with the source were marked for further review. Each item was rated using a four-level equivalence scale adapted from Hall et al. (2018) [10]:
A: Exact semantic match with the original wording and intent
B: Minor lexical differences with no impact on meaning
C: Conceptual meaning retained, but wording diverged significantly
D: Semantic and conceptual mismatch requiring retranslation
For items rated C or D, the translation lead proposed alternative translations and discussed the B-rated items with the committee. Prior to the committee review, all members received a detailed report outlining the discrepancies, the rationale behind the ratings, and the proposed alternatives. This comparison led to further refinements of several items. The rating scale and 7 questionnaire items were deemed to have perfect equivalence (A). Nineteen items were considered to have satisfactory equivalence (B), most of the time, they were just individual words like “hard” and “difficult” (“schwierig”). The introduction retained its conceptual meaning but lacked semantic precision and was therefore rated C. No items were assigned the lowest rating (D), indicating that all items showed at least some level of agreement.
Step 4: Committee review
A review committee examined the forward and back translations against the original to resolve inconsistencies. A detailed translation report documented all steps and discrepancies. The committee included the translation lead, the forward translation reviewer, and a linguist with expertise in semantic equivalence. Although the original developer was not fluent in German, they were available for clarification.
Items with cultural or semantic challenges were reviewed in depth, and alternative phrasings were explored. Revised items were back-translated and re-evaluated by the committee. No discrepancies were found in the second back translation, confirming semantic alignment. The rigorous multi-step process ensured strong comparability between the German and English versions, which was then approved for field testing.
Step 5: Field testing
To evaluate the feasibility and clarity of the translated HEAR-QL questionnaire, cognitive interviews were conducted with children with hearing loss. Cognitive interviewing is a qualitative method used to assess whether questionnaire items are understood as intended in the target language [5]. According to established guidelines, an appropriate sample size for this type of evaluation ranges from 8 to 20 participants. For this study, ten children aged 9;0 to 12;11 years were recruited through the Cochlear Implant Center and the Landesförderzentrum Schleswig. All participants had uni- or bilateral hearing loss and were fitted with cochlear implants (CI) or hearing aids (HA) for at least one year. Ethical approval was obtained from the Institutional Review Board of the Faculty of Human Sciences at the University of Applied Sciences Hamburg (HAW), EPHF0128, and written informed consent was collected prior to participation.
Eligibility criteria were largely aligned with those used in the original validation study [5]. Participants were required to have sufficient proficiency in spoken and written German to ensure meaningful engagement during the interviews. Convenience sampling was employed by inviting children who had scheduled appointments, thereby minimizing participant burden.
Interviews were conducted face-to-face using a semi-structured format. Children were encouraged to verbalize their thoughts while completing the questionnaire and to rephrase items in their own words.
The interviewer prompted participants to identify any confusing or ambiguous items and to share observations about the questionnaire’s clarity and relevance. In terms of audiological profile, the initial sample included five children with mild hearing loss (10–39 dB), four with moderate to moderately severe hearing loss (40–69 dB), and one child with profound hearing loss (90–120 dB). Eight children used bilateral hearing aids, one used a unilateral hearing aid, and one was equipped with bilateral cochlear implants.
Analysis of the first round of interviews revealed that several children had difficulty understanding specific items. In response, the questionnaire was revised using simplified language. Two items assessing the same construct were merged, and comparative (e.g., “…als Deine Freunde…”) was linguistically simplified by an expert in simple language. The resulting version comprised 25 items written in plain language. To evaluate the revised version, a second round of cognitive interviews was conducted with four additional children aged 7 to 12 years (see Table 1 [Tab. 1]). Feedback from this group confirmed improved clarity and comprehension across all items.
Table 1: Demographic characteristics of the study sample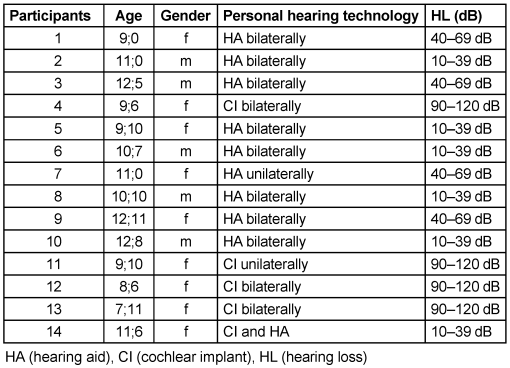
The iterative testing process demonstrated that cognitive interviewing is a valuable tool for refining pediatric PROMs. The final German version of the HEAR-QL showed strong comprehensibility and cultural appropriateness for school-aged children with hearing loss. During the cognitive interviews, the interviewer recorded detailed field notes capturing participants’ responses, reactions, and verbalized thoughts. These notes were transcribed and organized into a summary chart for systematic analysis. Comments indicating comprehension difficulties or misinterpretations were highlighted. For each questionnaire item, the frequency and nature of reported issues were assessed. Items flagged by at least one participant were reviewed by the committee. If consensus was reached that revisions were necessary, alternative phrasings were proposed, back-translated, and re-evaluated until agreement was achieved.
After the initial round of ten interviews, it became evident that more than half of the participants struggled with specific items. In particular, syntactic complexity posed a barrier to understanding. For example, the item: “Wenn du jemanden nicht hören kannst, fällt es dir schwer, ihn zu bitten, lauter zu sprechen oder das Gesagte zu wiederholen?” (“If you can’t hear someone, do you have a hard time asking them to speak louder or repeat what they said?”) was perceived as too complex. In consultation with the original developer, the sentence was reformulated to: “Wenn du jemanden nicht hören kannst, ist es schwierig für dich, ihn zu bitten, lauter zu sprechen oder das Gesagte zu wiederholen?” (“If you can’t hear someone, it is difficult for you to ask them to speak louder or to repeat what they said?”). Based on participant feedback, the committee revised the wording of four additional items. These changes were again subjected to back translation and committee review to ensure semantic fidelity.
To evaluate the revised version, a second round of cognitive interviews was conducted with the original ten participants and four additional children. This review confirmed that the questionnaire was now clearly understandable and appropriately formulated for the target age group. One redundant item was removed, resulting in a final total of 25 items (21. Does your hearing loss make you feel different from everyone else? – 26. Do you feel different from others because of your hearing?). This decision aligns with the Dutch adaptation of the HEAR-QL, which also reduced the item count [11]. The consolidated version was subsequently submitted to the committee for final approval.
Step 6: Finalization
The complete adaptation process of the HEAR-QL questionnaire—now comprising 25 items—was systematically documented using a modified version of the translation protocol outlined by Hall et al. (2018) [10]. All item iterations, committee discussions, and revision decisions were recorded in detail and archived for transparency and reproducibility. The finalized German version was meticulously proofread and formatted to preserve the structure, layout, and stylistic conventions of the original English-language instrument, ensuring visual and functional consistency across versions.
Discussion
The cross-cultural adaptation of the HEAR-QL questionnaire revealed notable challenges in achieving semantic and contextual equivalence. Despite efforts to preserve the original meaning, certain concepts proved difficult to translate due to linguistic and cultural differences. Emotionally nuanced or idiomatic terms, such as “nervous”, lacked direct equivalents in German that would be equally accessible to children with hearing loss. In such cases, compromises were necessary, which inevitably limited the degree of linguistic and conceptual fidelity.
The forward and backward translation procedures were instrumental in identifying discrepancies and ensuring content validity. However, they also highlighted the inherent complexity of the questionnaire and the difficulty of adapting certain expressions for a pediatric population. Field testing provided valuable feedback on how children perceived and understood the items, but the small sample size—limited to fourteen participants from a single cochlear implant center—restricted the diversity and representativeness of the findings. A broader, more heterogeneous sample would likely yield more robust insights into the questionnaire’s comprehensibility and applicability.
Some participants offered comments that extended beyond the scope of the current study. While these insights were valuable, they could not be fully integrated into the present adaptation process. Additionally, certain items remained difficult for children to understand, and in some cases, no suitable alternatives could be identified. This underscores the inherent challenge of adapting a complex instrument for children with hearing loss. The decision to remove one item was based on qualitative considerations during the translation and adaptation process; however, future validation studies should further examine whether item reduction is best guided by psychometric evidence.
A limitation of the present study is the absence of statistical analyses, which will be addressed in a subsequent validation study with a larger and more diverse sample. Overall, the adaptation process highlighted the complexity of the original HEAR-QL and the need for further refinement to enhance accessibility. A validation study of the adapted German version is currently underway. Future research should aim to test the instrument with larger and more diverse samples to establish broader validity and reliability.
Conclusion
This study underscores both the potential benefits and inherent challenges of adapting assessment tools for children with hearing loss. The cross-cultural adaptation process—including forward and backward translation and field testing—offered valuable insights into the linguistic and cultural complexities of transferring the instrument into a new context. While the adapted version preserved the overall intent of the original, certain terms lacked direct equivalents in German, and some items were difficult for children to interpret accurately.
The small, homogenous samplelimited the generalizability of the findings. Nevertheless, the results highlight the importance of carefully adapting assessment instruments to ensure accessibility and comprehensibility for children with special communication needs.
Notes
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank all participants, families, and the clinical staff involved in this study.
Competing interests
The authors declare that they have no competing interests.
References
[1] Stevenson J, Kreppner J, Pimperton H, Worsfold S, Kennedy C. Emotional and behavioural difficulties in children and adolescents with hearing impairment: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2015 May;24(5):477-96. DOI: 10.1007/s00787-015-0697-1[2] Theunissen SC, Rieffe C, Netten AP, Briaire JJ, Soede W, Kouwenberg M, Frijns JH. Self-esteem in hearing-impaired children: the influence of communication, education, and audiological characteristics. PLoS One. 2014 Apr 10;9(4):e94521. DOI: 10.1371/journal.pone.0094521
[3] Piva de Freitas P, Freire de Castro R, de Morais E Oliveira AP, Takahiro Chone C, Menino Castilho A. Quality of life in children with unilateral hearing loss undergoing cochlear implantation: A systematic review and meta-analysis. Braz J Otorhinolaryngol. 2025 Sep-Oct;91(5):101628. DOI: 10.1016/j.bjorl.2025.101628
[4] Ensing AE, Yang AF, Kallogjeri D, Lieu JEC. Factors Associated With Hearing-Related Quality of Life in Children With Hearing Loss. Laryngoscope. 2025 Sep;135(9):3382-8. DOI: 10.1002/lary.32193
[5] Jiménez Montesdeoca DDP, Falcón González JC, Borkoski Barreiro SA, Ramos Macías AM. Health-related quality of life perspectives of cochlear implanted children, their hearing peers, and their parents: a prospective case-control study. Am J Otolaryngol. 2025 Jul-Aug;46(4):104652. DOI: 10.1016/j.amjoto.2025.104652
[6] Smit AL, Burgers YRW, Swanenburg de Veye HFN, Stegeman I, Breugem CC. Hearing-related quality of life, developmental outcomes and performance in children and young adults with unilateral conductive hearing loss due to aural atresia. Int J Pediatr Otorhinolaryngol. 2021 Mar;142:110590. DOI: 10.1016/j.ijporl.2020.110590
[7] Weldring T, Smith SM. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv Insights. 2013 Aug 4;6:61-8. DOI: 10.4137/HSI.S11093
[8] Rachakonda T, Jeffe DB, Shin JJ, Mankarious L, Fanning RJ, Lesperance MM, Lieu JE. Validity, discriminative ability, and reliability of the hearing-related quality of life questionnaire for adolescents. Laryngoscope. 2014 Feb;124(2):570-8. DOI: 10.1002/lary.24336
[9] Umansky AM, Jeffe DB, Lieu JE. The HEAR-QL: quality of life questionnaire for children with hearing loss. J Am Acad Audiol. 2011 Nov-Dec;22(10):644-53. DOI: 10.3766/jaaa.22.10.3
[10] Hall DA, Zaragoza Domingo S, Hamdache LZ, Manchaiah V, Thammaiah S, Evans C, Wong LLN; International Collegium of Rehabilitative Audiology and TINnitus Research NETwork. A good practice guide for translating and adapting hearing-related questionnaires for different languages and cultures. Int J Audiol. 2018 Mar;57(3):161-75. DOI: 10.1080/14992027.2017.1393565
[11] Batthyany C, Schut AR, van der Schroeff M, Vroegop J. Translation and validation of the speech, spatial, and qualities of hearing scale (SSQ) and the hearing environments and reflection on quality of life (HEAR-QL) questionnaire for children and adolescents in Dutch. Int J Audiol. 2023 Feb;62(2):129-37. DOI: 10.1080/14992027.2021.2020914

