Monoclonal outbreak caused by ceftazidime-avibactam resistant blaOXA-48-positive, carbapenem-resistant Klebsiella pneumoniae in an intensive care unit
Bahise Çağla Taşkın Dalgıç 1Elif Seren Tanriverdi 2
İlayda Budak 3
Gülgün Yenişehirli 3
Barış Otlu 2
1 Microbiology Laboratory Unit, Manisa Public Health Laboratory, Manisa, Turkey
2 Department of Medical Microbiology, Inonu University, Faculty of Medicine, Malatya, Turkey
3 Department of Medical Microbiology, Tokat Gaziosmanpasa University, Faculty of Medicine, Tokat, Turkey
Abstract
Purpose: This study aimed to determine the ceftazidime-avibactam susceptibilities and clonal relationships of blaOXA-48-positive, carbapenem-resistant K. pneumaniae (CRKP) isolates.
Methods: Fifteen K. pneumaniae isolates from various clinical samples, determined as blaOXA-48-positive CRKP by VITEK 2 compact system and multiplex PCR, were included in the study. Colistin susceptibility of isolates was tested using the broth microdilution method. The Kirby-Bauer disk diffusion test was performed for CAZ-AVI susceptibility. Arbitrary primer sequence-based PCR (AP-PCR) was used to investigate genotypic similarity between the isolates.
Results: All 15 blaOXA-48-positive CRKP isolates were resistant to meropenem, ertapenem, imipenem, amikacin, gentamicin, ciprofloxacin and levoflokxacin. Four of the CRKP isolates were susceptible to SXT and colistin. 73.3% (11/15) of the CRKP isolates were found to be resistant to CAZ-AVI. One of the 15 blaOXA-48-positive CRKP isolates was also a blaNDM carrier. AP-PCR revealed that 15 isolates showed five different genotypes. Eleven of the isolates were classified under genotype 1, leading to a clustering rate of 73.3%. Isolates in the genotype 1 group were defined as outbreak isolates. All but one of the genotype 1 outbreak isolates were resistant to all antibiotics studied, including CAZ-AVI and colistin.
Conclusion: This study evaluated an intensive care unit outbreak caused by a clone resistant to CAZ-AVI, which has been reported to have susceptibility rates of up to 100% in OXA-48-producing CRKP isolates and is suggested as first choice therapy. To prevent the spread of CAZ-AVI-resistant CRKP isolates, it is essential to conduct active surveillance studies in hospitals. Especially ICUs – where these strains are common – should be routinely screened. Infection control practices in general must also be tightened.
Keywords
Carbapenem-resistant K. pneumoniae, ceftazidime-avibactam, hospital outbreak, intensive care unit, OXA-48
Introduction
Globally, the spread of carbapenem-resistant K. pneumoniae (CRKP) is rapidly increasing, and carbapenemase types vary between countries and regions. Among the carbapenemase types in K. pneumoniae isolates, KPC continues to be an endemic species in many parts of the world, especially in the USA [1], [2]. In Turkey, unlike the rest of the world, OXA-48-producing K. pneumoniae strains have been dominant for many years [3], [4]. Investigation of carbapenemase production and determination of its type in a CRKP isolate are very important in deciding which drug to choose for treatment [5]. To solve the resistance problem in Gram negative pathogens, new beta-lactamase inhibitors have been combined with known cephalosporins. The resulting ceftazidime-avibactam (CAZ-AVI) has shown significant in-vitro activity on CRKP isolates due to its broad enzyme inhibition effect, for instance, on OXA-48, KPC, ESBL and Amp C, but not MBL [5], [6].
In the IDSA 2023 guideline for treatment of Gram-negative infections, ceftazidime-avibactam is recommended for use in the treatment of infections other than those of the urinary tract, due to carbapenem-resistant Enterobactericeae (CRE). The same guideline states that the most common possibility of resistance development among new beta-lactams under treatment is again CAZ-AVI [7]. Global and regional resistance data report CAZ-AVI susceptibility rates as high as 100% in MBL-negative Enterobacteriaceae isolates [8], [9]. Among the studies investigating the molecular mechanisms of CAZ-AVI resistance in CRE isolates, blaKPC gene mutations are the most commonly reported. There are also rare reports about the CAZ-AVI resistance associated with the blaOXA-48 gene [10].
OXA-48 producing CRKP was first demonstrated in Turkey [11]. In later years, OXA-48 spread rapidly among K. pneumoniae strains via plasmids and was detected in many regions of the world, becoming the dominant type in some regions [12], [13]. Conducting surveillance studies showing clonal relationships between bacteria that are not usually included in laboratory routines is extremely important to predict and prevent outbreaks caused by these strains [14]. Due to the prevalence of OXA-48-producing isolates in Turkey, the purpose of this study was to determine CAZ-AVI susceptibility in blaOXA-48-positive CRKP isolates in order to shed light on treatment approaches, contribute to the epidemiological data of the world and our region, and provide data for studies to investigate the role of changes in the blaOXA-48 gene in CAZ-AVI resistance. An examination of the CAZ-AVI susceptibility of blaOXA-48-positive CRKP isolates grown in the laboratory of our hospital in 2020 showed a resistance rate that was quite high compared to Turkish and international data. We suspected that this was a monoclonal outbreak and aimed to perform clonal analysis on CRKP isolates.
Materials and methods
Selection of isolates
Fifteen K. pneumoniae isolates grown in the Microbiology Laboratory of Tokat Gaziosmanpasa University Hospital in 2020, were determined as blaOXA-48-positive CRKP by the VITEK 2 compact system and multiplex PCR and were included in the study.
Antimicrobial susceptibility testing
Susceptibility to ertapenem, imipenem, meropenem, amikacin, gentamicin, cipro/levofloxacin, and trimethoprim-sulfamethoxazole (SXT) was determined with the VITEK-2 (bioMérieux, France) automated system. The broth microdilution method was used to investigated colistin susceptibility. Ceftazidime-avibactam susceptibilities of the isolates were tested using the Kirby-Bauer disk diffusion method with a 10/4-µg ceftazidime-avibactam disk. Escherichia coli ATCC 25922 was used as the control strain. The CAZ-AVI sensitivity results were evaluated according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) v14.0 guideline.
Molecular detection of carbapenemase genes
DNA of CRKP isolates was extracted with the QIAamp DNA midi kit (Qiagen, Hilden, Germany). Detection of of blaOXA-48, blaNDM, blaKPC, blaIMP and blaVIM genes was performed by in-house multiplex PCR according to the standard conditions and primer sequences previously described [15]. GeneAmp PCR System 9700 (Applied Biosystems, Waltham, MA, USA) thermocycler system used for DNA amplification. Gel electrophoresis was used to visualize amplification products.
Investigation of clonal relationships between isolates
The arbitrary primer sequence-based PCR (AP-PCR) method was used in clonal analysis of the isolates. For AP-PCR, first, 50 µl of reaction mixture including M13 primer (5’-GAGGGTGGCGGTTCT-3’) was prepared. Subsequently, amplification products were obtained with the Thermal Cycler GeneAmp PCR System 9700 (Applied Biosystems, Waltham, MA, USA) under the operating conditions described previously [16]. GelCompar II software (version 6.5; Applied Maths, Sint-Martens-Latem, Belgium) was used for band profile analysis. Cluster analysis was performed with UPGMA (Unweighted pair group method with arithmetic mean). Isolates with a Dice similarity coefficient above 95% were determined as the same genotype. If this coefficient was between 85% and 95%, the isolates were defined as subtypes of the same strain. Isolates with similarity rates below 85% were evaluated as genotypically different.
Ethical approval
Approval of Tokat Gaziosmanpasa University Faculty of Medicine Ethics Committee (No:23-KAEK-282) was granted on 19.12.2023.
Results
Distrubition of samples
Of the CRKP, 80% (12/15) were isolated from the intensive care unit (ICU), and 20% (3/15) from the ward. The distribution of the isolates according to department is shown in Table 1 [Tab. 1]. The majority of the isolates were taken from blood samples 40%. This was followed by urinary system samples, with 33.3%, and sputum with 26.7%.
Table 1: Distrubition of samples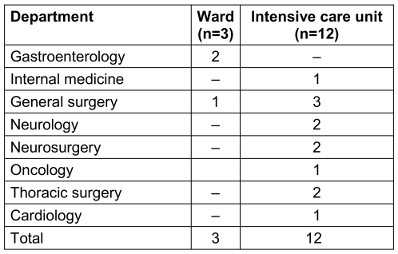
Carbapenemase gene and antimicrobial susceptibility testing results
One of the 15 blaOXA-48-positive CRKP isolates was also a blaNDM carrier. All 15 blaOXA-48-positive CRKP isolates were resistant to meropenem and imipenem, amikacin, gentamicin, ciprofloxacin, and levofloxacin. Four (26.7%) CRKP isolates were susceptible to SXT and colistin. 73.3% (11/15) of the blaOXA-48-positive CRKP isolates were determined to be resistant to CAZ-AVI. Three of the four isolates susceptible to CAZ-AVI, SXT and colistin were isolated from patients staying in the ward. All 11 isolates resistant to CAZ-AVI were isolated from intensive care unit patients.
Clonal relationship results
According to AP-PCR results, 15 isolates showed 5 different genotypes. It was determined that the clustered isolates belonged to a single distinct cluster (with a tolerance of 1.0, an optimization of 1.0, and a limit value of 85%). Eleven of the isolates were classified under genotype 1, leading to a clustering rate of 73.3%. Isolates in the genotype 1 group were defined as outbreak isolates. Figure 1 [Fig. 1] shows the gel electrophoresis images and dendrogram of the isolates.
Figure 1: Gel electrophoresis results and dendrogram of the isolates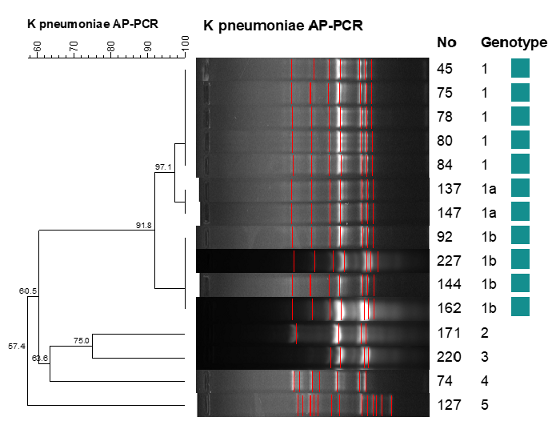
One of the outbreak isolates was a blaOXA-48 + blaNDM carrier. Six of the genotype 1 isolates caused an outbreak in the ICU in January through March, 2020. Four isolates were isolated in June through August, 2020. Three of these were isolated from intensive care unit patients, and one was isolated from a patient in the general surgery ward. However, this patient was transferred to the ward after staying in the general surgery ICU for 12 days. Of the four isolates that were not outbreak isolates (genotype 2, 3, 4, 5), two were isolated from ward patients and two from ICU patients (Figure 2 [Fig. 2]).
Figure 2: Arbitrarily primed polymerase chain reaction (AP-PCR) results of blaoxa-48-positive carbapenem-resistant K. pneumoniae isolates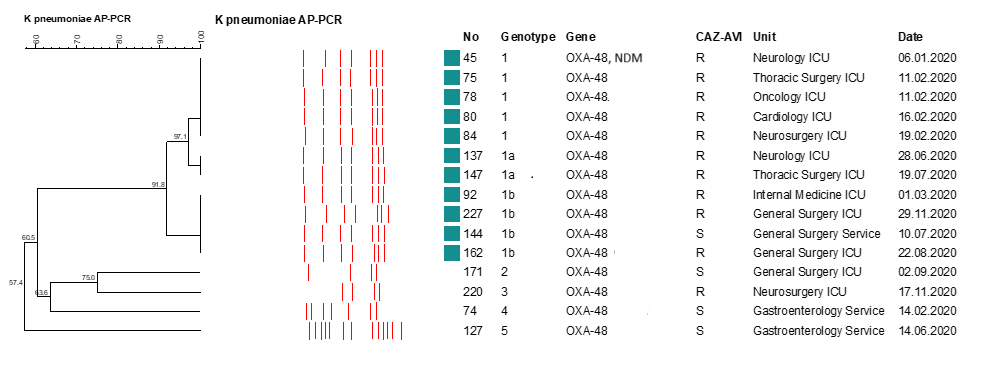
Ten (90.9%) of the outbreak isolates were resistant to all antibiotics tested, including CAZ-AVI and colistin. One of the outbreak isolates was found to be susceptible to CAZ-AVI. Three of the four isolates which were not outbreak isolates were found to be sensitive to CAZ-AVI, while one of them was resistant. The antimicrobial susceptibility profile and genotypic pattern of the isolates are shown in Table 2 [Tab. 2].
Table 2: Antimicrobial susceptibility profile and genotypic pattern of the isolates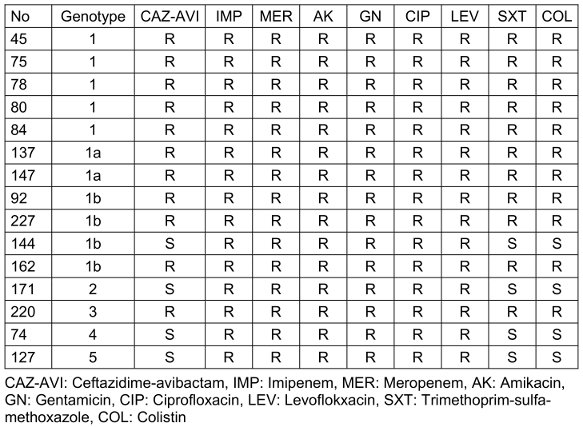
Discussion
While almost all Enterobactericeae strains were sensitive to carbapenems in the early 2000s, sensitivity rates have decreased to 50% currently, varying between regions and countries [17]. Epidemiological studies show that CRKP constitutes a significant majority of CRE isolates. In the CRACKLE-2 cohort study conducted in the USA, 57% of CRE isolates were CRKP [18]. Similarly, in a study by Wang et al. in China, 1,201 of 1,801 CRE isolates were CRKP [19]. The European antimicrobial resistance surveillance report of 2023 showed that CRKP isolates in Turkey increased from 32.5% to 49.1% in 4 years [20].
Carbapenemase production in CRKP isolates is the first-line resistance mechanism in the development of carbapenem resistance. Globally, the most common carbapenemases produced in CRKP isolates are KPC, NDM and OXA-48 [17], [18], [19]. KPC-producing CRKP isolates are endemic in many countries, especially in the USA, Brazil, China and Greece [1], [17], [18], [19]. Rocha et al. detected the blakpc gene in 94.7% of CRKP isolates in Brazil and Tsilipounidaki et al. detected the blaKPC gene in 75% of K. pneumoniae isolates in Greece [21], [22]. In contrast, epidemiological data in Turkey showed that OXA-48 was the most common carbapenemase in CRKP isolates. In a study within the scope of the European Survey on Carbapenemase Producing Enterobacteriaceae (EuSCAPE) project, the OXA-48 gene was detected in 83.1% of CRKP isolates in Turkey [4]. Subsequently, 6.5% NDM, 3.2% VIM, 2.4% OXA-48+NDM and 2.4% OXA-48+VIM were found. No KPC-positive isolates were detected in that study [4].
The rapid increase in CRE globally has created a need for new drug options in treatment. The new beta-lactam-beta-lactamase inhibitor complex ceftazidime-avibactam is used in systemic infections caused by CRE [7]. Studies investigating the in-vitro activity of CAZ-AVI on CRE isolates reported high susceptibility rates in MBL-negative carbapenem-resistant isolates. According to the INFORM global surveillance report, between 2015 and 2017, the susceptibility rate to caz-avi in carbapenemase-positive MBL-negative Enterobacteriaceae isolates was 99.8% [8]. In a recent study the susceptibility of ceftazidime to avibactam was reported as 84.2% in CRE isolates. In that study, 97.8% of KPC positive isolates, 69.2% of OXA-48 positive isolates, 2.6% of MBL positive isolates and 96% of carbapenemase non-producers were found to be susceptible to CAZ-AVI. It was stated that all OXA-48 positive isolates that were resistant to caz-avi were also MBL carriers [23]. In Turkey, Arici et al. [24] found an 89.3% rate of CAZ-AVI sensitivity in CRKP isolates. This increased to 100% in CRKPs that produce only OXA-48. It was determined that all CAZ-AVI resistant isolates were OXA-48+ NDM carriers [24]. In our study, 11 (73.3%) of 15 blaOXA-48-positive CRKP isolates were determined to be resistant to CAZ-AVI. Moreover, only one of them was a carrier of NDM. Our findings differ from global data and Turkey overall, the authors suspected that this was a monoclonal CAZ-AVI-resistant blaOXA-48-positive CRKP outbreak. The AP-PCR results presented here confirm this.
Hospital outbreaks of OXA-48-producing CRKP have been reported in many countries around the world. The majority of these were caused by strains isolated from patients in ICUs. The long stay of patients infected with multidrug-resistant strains in ICUs constitutes one of the predisposing factors for outbreaks caused by these resistant strains. Ten of the 11 outbreak isolates in our study were isolated from ICU patients. One isolate was from a patient transferred from the ICU to the ward. An outbreak of colistin and CRKP ST307, which produces both NDM and OXA-48, was reported in Germany in 2019 [25]. Sharma et al. [26] reported a hospital outbreak caused by 2 different sequence type clones, 56.25% of which were blaoxa-48 and blandm producing colistin-resistant CRKP isolates. They stated that the outbreak started in the ICU. Guducuoglu et al. [27] reported a high mortality hospital outbreak in Turkey caused by colistin-resistant-, NDM- and OXA-48- positive ST11-type CRKP. These studies did not mention the CAZ-AVI susceptibility profile of the isolates. In Turkey, Arici et al. [24] reported an outbreak of OXA-48-producing CRKP originating from a single clone; all of the isolates here were susceptible to CAZ-AVI. In our study, 10 (90.9%) of the genotype 1 outbreak isolates were resistant to all antibiotics studied, including CAZ-AVI and colistin.
Studies investigating CAZ/AVI resistance in OXA-48-producing CRKP isolates are quite limited. In a few studies, Pro68Ala and Tyr211Ser amino acid substitutions were held responsible for the decreased CAZ/AVI susceptibility in these strains. It was shown that the variant enzyme had a high ability to hydrolyze CAZ, while the inhibitory effect of AVI was reduced [28].
Our study is remarkable in terms of the hospital outbreak of the blaOXA-48-positive CRKP clone resistant to CAZ-AVI, which is recommended as the first choice in the treatment of CRKP infections, with reported sensitivity rates of up to 100% in OXA-48-producing CRKP. Determination of phenotypic and genotypic resistance types in hospitals is crucial for selecting treatment strategies.
In our hospital, in addition to routine infection control measures, when an increase in the frequency of an infection caused by a single microorganism with a similar antibiotic resistance profile is noticed, infection control measures are tightened. This includes increasing patient isolation measures, providing training to staff and preventing staff reassignment, and increasing the frequency of hospital environment and equipment disinfection. CAZ-AVI began to be used in Turkey on April 28, 2021. Ceftazidime-avibactam was not used in our hospital in 2020. In addition, clonal analysis and molecular resistance gene analysis are not performed routinely for bacteria. Therefore, a limitation of the present study is that active surveillance was not performed and the data were evaluated retrospectively.
Conclusion
Determination of phenotypic and genotypic resistance types in hospitals is important for determing appropriate treatment strategies. It is very important to conduct active surveillance studies in hospitals to prevent the spread of CAZ-AVI-resistant CRKP isolates. In addition, it is essential to routinely screen samples from ICUs, where these strains are common, and implement strict infection control programs.
Notes
Authors’ ORCIDs
- Taskin Dalgiç BÇ: 0000-0002-1271-7522
- Tanriverdi ES: 0000-0002-0449-0356
- Budak I: 0009-0004-3681-859X
- Yenisehirli G: 0000-0001-7030-0752
- Otlu B: 0000-0002-6220-0521
Funding
None.
Competing interests
The authors declare that they have no competing interests.
References
[1] Ma J, Song X, Li M, Yu Z, Cheng W, Yu Z, Zhang W, Zhang Y, Shen A, Sun H, Li L. Global spread of carbapenem-resistant Enterobacteriaceae: Epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023 Jan;266:127249. DOI: 10.1016/j.micres.2022.127249[2] Nordmann P, Poirel L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin Infect Dis. 2019 Nov 13;69(Suppl 7):S521-S528. DOI: 10.1093/cid/ciz824
[3] Kutlu HH, Us E, Tekeli A. Bir üniversite hastanesinde 2010-2014 yılları arasında izole edilen Enterobacteriaceae türlerinin karbapenemaz genlerinin araştırılması ve moleküler epidemiyolojisinin belirlenmesi [Investigation of carbapenemase genes and molecular epidemiology of Enterobacteriaceae strains isolated between 2010-2014 in a university hospitals]. Mikrobiyol Bul. 2018 Jan;52(1):1-12. Turkish. DOI: 10.5578/mb.66156
[4] Çakar A, Akyön Y, Gür D, Karatuna O, Öğünç D, Özhak Baysan B, et al. Türkiye’de 2014 yılı içinde izole edilen karbapeneme dirençli Escherichia coli ve Klebsiella pneumoniae izolatlarında karbapenemaz varlığının araştırılması [Investigation of carbapenemases in carbapenem-resistant Escherichia coli and Klebsiella pneumoniae strains isolated in 2014 in Turkey]. Mikrobiyol Bul. 2016 Jan;50(1):21-33. DOI: 10.5578/mb.10695
[5] Doi Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin Infect Dis. 2019 Nov 13;69(Suppl 7):S565-S575. DOI: 10.1093/cid/ciz830
[6] Karlowsky JA, Kazmierczak KM, Bouchillon SK, de Jonge BLM, Stone GG, Sahm DF. In Vitro Activity of Ceftazidime-Avibactam against Clinical Isolates of Enterobacteriaceae and Pseudomonas aeruginosa Collected in Asia-Pacific Countries: Results from the INFORM Global Surveillance Program, 2012 to 2015. Antimicrob Agents Chemother. 2018 Jun 26;62(7):e02569-17. DOI: 10.1128/AAC.02569-17
[7] Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clin Infect Dis. 2024 Aug 7:ciae403. DOI: 10.1093/cid/ciae403
[8] Spiliopoulou I, Kazmierczak K, Stone GG. In vitro activity of ceftazidime/avibactam against isolates of carbapenem-non-susceptible Enterobacteriaceae collected during the INFORM global surveillance programme (2015-17). J Antimicrob Chemother. 2020 Feb 1;75(2):384-91. DOI: 10.1093/jac/dkz456
[9] Zhang P, Shi Q, Hu H, Hong B, Wu X, Du X, Akova M, Yu Y. Emergence of ceftazidime/avibactam resistance in carbapenem-resistant Klebsiella pneumoniae in China. Clin Microbiol Infect. 2020 Jan;26(1):124.e1-124.e4. DOI: 10.1016/j.cmi.2019.08.020
[10] Xiong L, Wang X, Wang Y, Yu W, Zhou Y, Chi X, Xiao T, Xiao Y. Molecular mechanisms underlying bacterial resistance to ceftazidime/avibactam. WIREs Mech Dis. 2022 Nov;14(6):e1571. DOI: 10.1002/wsbm.1571
[11] Poirel L, Héritier C, Tolün V, Nordmann P. Emergence of oxacillinase-mediated resistance to imipenem in Klebsiella pneumoniae. Antimicrob Agents Chemother. 2004 Jan;48(1):15-22. DOI: 10.1128/AAC.48.1.15-22.2004
[12] Lee YL, Ko WC, Hsueh PR. Geographic patterns of global isolates of carbapenem-resistant Klebsiella pneumoniae and the activity of ceftazidime/avibactam, meropenem/vaborbactam, and comparators against these isolates: Results from the Antimicrobial Testing Leadership and Surveillance (ATLAS) program, 2020. Int J Antimicrob Agents. 2022 Nov-Dec;60(5-6):106679. DOI: 10.1016/j.ijantimicag.2022.106679
[13] Castanheira M, Doyle TB, Collingsworth TD, Sader HS, Mendes RE. Increasing frequency of OXA-48-producing Enterobacterales worldwide and activity of ceftazidime/avibactam, meropenem/vaborbactam and comparators against these isolates. J Antimicrob Chemother. 2021 Nov 12;76(12):3125-34. DOI: 10.1093/jac/dkab306
[14] Duman Y, Ersoy Y, Gursoy NC, Altunisik Toplu S, Otlu B. A silent outbreak due to Klebsiella pneumoniae that co-produced NDM-1 and OXA-48 carbapenemases, and infection control measures. Iran J Basic Med Sci. 2020 Jan;23(1):46-50. DOI: 10.22038/IJBMS.2019.35269.8400
[15] Poirel L, Walsh TR, Cuvillier V, Nordmann P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011 May;70(1):119-23. DOI: 10.1016/j.diagmicrobio.2010.12.002
[16] Kuzucu C, Durmaz R, Otlu B, Aktas E, Gulcan H, Cizmeci Z. Species distribution, antifungal susceptibility and clonal relatedness of Candida isolates from patients in neonatal and pediatric intensive care units at a medical center in Turkey. New Microbiol. 2008 Jul;31(3):401-8.
[17] Doi Y, Paterson DL. Carbapenemase-producing Enterobacteriaceae. Semin Respir Crit Care Med. 2015 Feb;36(1):74-84. DOI: 10.1055/s-0035-1544208
[18] van Duin D, Arias CA, Komarow L, Chen L, Hanson BM, Weston G, Cober E, Garner OB, Jacob JT, Satlin MJ, Fries BC, Garcia-Diaz J, Doi Y, Dhar S, Kaye KS, Earley M, Hujer AM, Hujer KM, Domitrovic TN, Shropshire WC, Dinh A, Manca C, Luterbach CL, Wang M, Paterson DL, Banerjee R, Patel R, Evans S, Hill C, Arias R, Chambers HF, Fowler VG Jr, Kreiswirth BN, Bonomo RA; Multi-Drug Resistant Organism Network Investigators. Molecular and clinical epidemiology of carbapenem-resistant Enterobacterales in the USA (CRACKLE-2): a prospective cohort study. Lancet Infect Dis. 2020 Jun;20(6):731-41. DOI: 10.1016/S1473-3099(19)30755-8
[19] Wang Q, Wang X, Wang J, Ouyang P, Jin C, Wang R, Zhang Y, Jin L, Chen H, Wang Z, Zhang F, Cao B, Xie L, Liao K, Gu B, Yang C, Liu Z, Ma X, Jin L, Zhang X, Man S, Li W, Pei F, Xu X, Jin Y, Ji P, Wang H. Phenotypic and Genotypic Characterization of Carbapenem-resistant Enterobacteriaceae: Data From a Longitudinal Large-scale CRE Study in China (2012-2016). Clin Infect Dis. 2018 Nov 13;67(suppl_2):S196-S205. DOI: 10.1093/cid/ciy660
[20] European Centre for Disease Prevention and Control; World Health Organization. Antimicrobial resistance surveillance in Europe 2023 - 2021 data. Stockholm: European Centre for Disease Prevention and Control and World Health Organization; 2023. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/Antimicrobial%20resistance%20surveillance%20in%20Europe%202023%20-%202021%20data.pdf
[21] Rocha VFD, Barbosa MS, Leal HF, Silva GEO, Sales NMMD, Monteiro ASS, Azevedo J, Malheiros ARX, Ataide LA, Moreira BM, Reis MG, Bahia FMM, Reis JN. Prolonged Outbreak of Carbapenem and Colistin-Resistant Klebsiella pneumoniae at a Large Tertiary Hospital in Brazil. Front Microbiol. 2022 Mar 9;13:831770. DOI: 10.3389/fmicb.2022.831770
[22] Tsilipounidaki K, Athanasakopoulou Z, Müller E, Burgold-Voigt S, Florou Z, Braun SD, Monecke S, Gatselis NK, Zachou K, Stefos A, Tsagalas I, Sofia M, Spyrou V, Billinis C, Dalekos GN, Ehricht R, Petinaki E. Plethora of Resistance Genes in Carbapenem-Resistant Gram-Negative Bacteria in Greece: No End to a Continuous Genetic Evolution. Microorganisms. 2022 Jan 13;10(1):159. DOI: 10.3390/microorganisms10010159
[23] Sader HS, Mendes RE, Duncan L, Kimbrough JH, Carvalhaes CG, Castanheira M. Ceftazidime-avibactam, meropenem-vaborbactam, and imipenem-relebactam activities against multidrug-resistant Enterobacterales from United States Medical Centers (2018-2022). Diagn Microbiol Infect Dis. 2023 Jun;106(2):115945. DOI: 10.1016/j.diagmicrobio.2023.115945
[24] Arıcı N, Tanrıverdi ES, Çalık Ş, Kansak N, Adaleti R, Otlu B, Aksaray S. Carbapenem-resistant Klebsiella pneumoniae outbreak with monoclonal spread: Evaluation of resistance genes and ceftazidime-avibactam susceptibility. Indian J Med Microbiol. 2023 Nov-Dec;46:100431. DOI: 10.1016/j.ijmmb.2023.100431
[25] European Centre for Disease Prevention and Control. Outbreak of carbapenemase-producing (NDM-1 and OXA-48) and colistin-resistant Klebsiella pneumoniae ST307, north-east Germany, 2019. 2019 Oct 28. ECDC: Stockholm; 2019. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/Klebsiella-pneumoniae-resistance-Germany-risk-assessment.pdf
[26] Sharma S, Banerjee T, Kumar A, Yadav G, Basu S. Extensive outbreak of colistin resistant, carbapenemase (blaOXA-48, blaNDM) producing Klebsiella pneumoniae in a large tertiary care hospital, India. Antimicrob Resist Infect Control. 2022 Jan 6;11(1):1. DOI: 10.1186/s13756-021-01048-w
[27] Guducuoglu H, Gursoy NC, Yakupogullari Y, Parlak M, Karasin G, Sunnetcioglu M, Otlu B. Hospital Outbreak of a Colistin-Resistant, NDM-1- and OXA-48-Producing Klebsiella pneumoniae: High Mortality from Pandrug Resistance. Microb Drug Resist. 2018 Sep;24(7):966-72. DOI: 10.1089/mdr.2017.0173
[28] Fröhlich C, Sørum V, Thomassen AM, Johnsen PJ, Leiros HS, Samuelsen Ø. OXA-48-Mediated Ceftazidime-Avibactam Resistance Is Associated with Evolutionary Trade-Offs. mSphere. 2019 Mar 27;4(2):e00024-19. DOI: 10.1128/mSphere.00024-19

