Active surveillance cultures for multidrug-resistant Gram-negative organisms in the intensive care unit: is it necessary to conduct them weekly?
Lorena Lima 1Elaine Alves 1
Bianca Santos 1
Adriana Assumpção 1
Priscila Oliveira 1
Priscilla Monteiro 1
Julia Mascarenhas 2
Clara Rizzo 3
Sérgio Morgado 4
Luiz Mascarenhas 1,2
1 Hospital Infection Control Committee, São Francisco na Providência de Deus Hospital, Rio de Janeiro, Brazil
2 Estácio de Sá University, Rio de Janeiro, Brazil
3 Federal University of the State of Rio de Janeiro, Rio de Janeiro, Brazil
4 Laboratory of Molecular Genetics of Microorganisms, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil
Abstract
Aim: Multidrug-resistant Gram-negative bacteria (MDR-GNB) pose a major threat to public health due to the limited treatment options and their frequent association with healthcare-associated infections. Active surveillance culture (ASC), a component of infection prevention strategies, remains controversial. This study evaluated the effectiveness of ASC performed weekly versus only upon ICU admission and discharge for detecting MDR-GNB.
Materials and methods: In a prospective study, two monitoring strategies were compared over a period of 18 months in six intensive care units. Phase 1 involved conducting ASC weekly, while Phase 2 entailed conducting ASC exclusively at the time of ICU admission and discharge.
Results: A total of 233 MDR-GNB infections were documented: 130 (11.38/1,000 patient-days) in Phase 1 and 103 (8.47/1,000 patient-days) in Phase 2. This reflects a statistically significant decrease in infection rates in Phase 2 (IRR: 1.34; 95% CI: 1.04–1.74). No significant differences were observed in species-specific infection rates between the two phases.
Conclusions: Reducing ASC frequency from weekly to only ICU admission and discharge did not increase MDR-GNB infection rates. The implementation of comprehensive infection prevention and control measures proved sufficient for the management of bacterial infections.
Keywords
contact precautions, ICU, infection, MDR, active surveillance culture
Introduction
Multidrug-resistant Gram-negative bacteria (MDR-GNB), including Acinetobacter (A.) baumannii (MDR-AB), Pseudomonas (P.) aeruginosa (MDR-PA) and carbapenem-resistant Enterobacteriaceae (CRE), represent pathogens that have become a significant global health concern due to their association with healthcare-associated infections [1], [2]. The paucity of effective treatment options engenders considerable challenges in the management of these infections [3]. Infection prevention and control (IPC) interventions have been implemented in many hospitals with a range of recommendations from committees and societies over the years. These interventions include disinfectant surface cleaning, strict control of antibiotic use, contact precautions), hand hygiene, and tracking or active search swabbing. However, the relative effectiveness of IPC is still inconclusive, especially in high-resistance endemic settings [4]. The active surveillance culture (ASC) program, a component of an infection prevention strategy, remains a subject of debate, and its benefits are contingent on factors such as the target population, the level of endemicity, and the integration of multifaceted strategies [5]. In particular, swab screening for the detection of asymptomatic colonization is laborious and has a low cost:benefit ratio. It also commonly produces false negatives, which increases the risk of contamination of other patients [6]. Therefore, we question the effectiveness of frequent ASC. The aim of this study was to evaluate the performance of ASC in an ICU by testing patients either weekly or only upon ICU admission and discharge.
Materials and methods
This study was conducted at the São Francisco na Providência de Deus Hospital (Rio de Janeiro/Brazil), a tertiary care hospital with 60 beds in six ICUs. For this study, IPC measures included contact precautions (gloves, aprons, caps, and/or glasses), thorough disinfectant surface cleaning, hand hygiene, and strict antibiotic use control. The study spanned a duration of 18 months, commencing in December 2020 and concluding in May 2022, and was divided into two phases, each spanning a period of nine months. Phase 1, serving as control, encompassed 11,425 patient days, during which all patients admitted to ICUs underwent weekly ASC for MDR-AB, MDR-PA, and CRE. Phase 2, spanning 12,153 patient days, introduced ASC exclusively upon patient admission and discharge. ASC was obtained from the oropharynx or rectum of patients. Regardless of phase, all patients, including those with negative results, were kept under IPC measures until ICU discharge. For Phase 2, the decision was made to take swabs only upon the patients' admission and discharge to determine whether the case was imported or autochthonous. Patients were considered infected if they had a positive result in clinical material (blood, urine, or tracheal aspirate). They were kept in isolation and under IPC interventions until they were discharged from the ICU. No substantial alterations in patient health status, hospital infrastructure, or infection prevention techniques occurred at any of the sites during the study period.
The overall infection rate and the rate of infection for each pathogen in all ICUs were determined monthly. The BD Phoenix™ Automated Microbiology System (Becton, Dickinson and Company, USA) was used to identify the species of bacteria obtained from infections in the ICUs and to profile their antibiotic susceptibility. For laboratory purposes, the minimum inhibitory concentration of ertapenem, imipenem, and meropenem was determined for all MDR-AB, MDR-PA, and CRE isolates from clinical material, in accordance with the Clinical and Laboratory Standards Institute guidelines. Bacteria resistant to at least one antimicrobial drug from at least three antibiotic classes were considered multidrug resistant (MDR). The Poisson or negative binomial distribution (in case of over-dispersed data) models were used to compare the rates of bacterial infections during the study phases using R software. The results were expressed as an incidence rate ratio (IRR) with their corresponding 95% confidence interval (95%-CI) values.
Results
We compared the infection rates of two patient cohorts under the same IPC measures (contact precautions, thorough disinfectant surface cleaning, hand hygiene, and strict antibiotic use control). The only variable was the frequency with which screening tests with swabs were performed. During the 18-month period of this study, there were 233 cases of MDR-GNB infections with 130 cases (55.7%) in Phase 1 and 103 (44.3%) in Phase 2. The overall infection rate per 1,000 patient-days was 11.38 (130/11,425) in Phase 1 and 8.47 (103/12,153) in Phase 2 (IRR: 1.34; CI 95% 1.04–1.74) (Table 1 [Tab. 1]). This is statistical evidence suggesting that Phase 1 had more infections per unit of time than Phase 2 for all MDR-GNB. Table I details the distribution of infections by species. Generally, there were no statistically significant differences between phases for individual species.
Table 1: Rates of MDR-GNB infections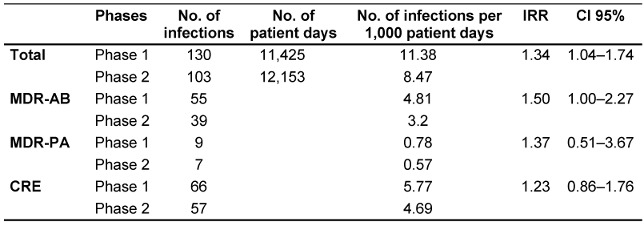
Discussion
The increasing burden of MDR-GNB infections has underscored the pressing need for effective prevention and control strategies. Although the implementation of ASC programs remains a subject of debate, it may offer certain advantages, contingent on specific variables [5]. A notable benefit of an ASC program is its capacity to identify colonized patients, enabling their enrollment in contact precautions to prevent cross-transmission. This approach optimizes more appropriate empirical therapy, leading to a reduction in mortality and selection pressure [7], [8]. However, the high frequency of false-negative ASC samples may lead to underestimation of the true burden of MDR-GNB, resulting in ineffective containment and inadequate initial therapy [6]. Other limitations include low sensitivity for cultures from certain sites, labor intensity, high cost of selective plates, administrative difficulties, and low standardization of ASC policies [9], [10].
This study evaluated the effectiveness of performing ASC weekly versus only upon patient admission and discharge from the ICU. We observed that reducing surveillance through ASC did not result in an increase in infection rates. In fact, when considering all MDR-GNB evaluated, statistical evidence of a reduction in infection rates was observed in Phase 2. However, this may be due to the reduced ASC screening in Phase 2. In any case, conducting additional swab tests did not affect the control of bacteria in the ICU. Therefore, implementing several infection control measures in both phases was effective. This makes it possible to optimize hospital staff functions and decrease costs. Although there may be additional costs for contact precaution items, this protocol reduces costs associated with swabs, labor for collection, and laboratory expenses. Indeed, these results were similar to a study considering methicillin-resistant Staphylococcus aureus in a neonatal intensive care unit [11]. Further studies on ASC are necessary to determine the applicability of these results to all types of bacteria and hospital environments or only in specific cases.
Based on these results, we have changed the periodicity of ASC from weekly to admission and discharge of patients, and we have maintained contact precautions for all patients in our hospital. The Infection Control Committee and hospital management endorsed this modification to the ASC protocol in September 2021, and it has since been established as an institutional policy. As of June 2025, the stability of our infection and transmission rates indicates the efficacy of these measures.
Limitations
This study has several limitations. First, it was conducted in a single tertiary hospital, which may limit the generalizability of the findings to other institutions or epidemiological settings. Second, only MDR-GNB (A. baumannii, P. aeruginosa, and CRE) were assessed, limiting applicability to other pathogens. Finally, the observation period of 18 months may not capture long-term epidemiological trends.
Conclusions
Reducing ASC frequency from weekly to only upon ICU admission and discharge did not increase MDR-GNB infection rates. The implementation of comprehensive infection prevention and control measures proved sufficient for the management of bacterial infections. This approach has been demonstrated to reduce costs and optimize resource allocation. Further studies are needed to generalize these findings to other settings and pathogens.
Notes
Competing interests
The authors declare that they have no competing interests.
Ethical approval
This study analyzed anonymized, aggregated data generated from the hospital’s routine infection prevention and control program. No patient-identifiable information was collected, and no additional procedures were performed for research purposes. According to Brazilian National Research Ethics Guidelines (CNS Resolution 466/12), such studies are exempt from ethics committee review.
Funding
This study was financed by FAPERJ - Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro, Processo SEI-260003/019688/2022.
Acknowledgments
We thank Fabiano R. Oliveira for administrative support.
Authors’ ORCIDs
- Lima L: https://orcid.org/0000-0003-3921-560X
- Alves E: https://orcid.org/0009-0006-2636-5835
- SantosB: https://orcid.org/0000-0001-6841-5104
- Mascarenhas J: https://orcid.org/0009-0007-0681-7758
- Rizzo C: https://orcid.org/0009-0000-3662-784X
- Morgado S: https://orcid.org/0000-0003-4877-7639
- Mascarenhas L: https://orcid.org/0000-0002-0500-1219
References
[1] Laxminarayan R, Duse A, Wattal C, Zaidi AK, Wertheim HF, Sumpradit N, et al. Antibiotic resistance-the need for global solutions. Lancet Infect Dis. 2013 Dec; 13(12):1057-98. DOI: 10.1016/S1473-3099(13)70318-9[2] Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, Cormican M, et al. Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. Lancet Infect Dis. 2013 Sep;13(9):785-96. DOI: 10.1016/S1473-3099(13)70190-7
[3] Karaiskos I, Giamarellou H. Multidrug-resistant and extensively drug-resistant Gram-negative pathogens: current and emerging therapeutic approaches. Expert Opin Pharmacother. 2014 Jul;15(10):1351-70. DOI: 10.1517/14656566.2014.914172
[4] Moodley P, Whitelaw A. The pros, cons, and unknowns of search and destroy for carbapenem-resistant enterobacteriaceae. Curr Infect Dis Rep. 2015 Jun;17(6):483. DOI: 10.1007/s11908-015-0483-8
[5] Thatrimontrichai A, Apisarnthanarak A. Active surveillance culture program in asymptomatic patients as a strategy to control multidrug-resistant gram-negative organisms: What should be considered? J Formos Med Assoc. 2020 Nov;119(11):1581-5. DOI: 10.1016/j.jfma.2019.08.015
[6] Teerawattanapong N, Kengkla K, Dilokthornsakul P, Saokaew S, Apisarnthanarak A, Chaiyakunapruk N. Prevention and control of multidrug-resistant Gram-negative bacteria in adult intensive care units: A systematic review and network meta-analysis. Clin Infect Dis. 2017 Nov 15;64(suppl_2):S51-60. DOI: 10.1016/j.jfma.2019.08.015
[7] Siegel JD, Rhinehart E, Jackson M, Chiarello L. Healthcare infection control practices advisory committee. management of multidrug-resistant organisms in health care settings, 2006. Am J Infect Control. 2007 Dec;35(10 Suppl 2):S165-93. DOI: 10.1016/j.ajic.2007.10.006
[8] Tacconelli E, Cataldo MA, Dancer SJ, De Angelis G, Falcone M, Frank U, et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin Microbiol Infect. 2014 Jan;20(Suppl 1):1-55. DOI: 10.1111/1469-0691.12427
[9] Adler A, Navon-Venezia S, Moran-Gilad J, Marcos E, Schwartz D, Carmeli Y. Laboratory and clinical evaluation of screening agar plates for detection of carbapenem-resistant Enterobacteriaceae from surveillance rectal swabs. J Clin Microbiol. 2011 Jun;49(6):2239-42. DOI: 10.1128/JCM.02566-10
[10] Zahar JR, Blot S, Nordmann P, Martischang R, Timsit JF, Harbarth S, et al. Screening for intestinal carriage of extended-spectrum beta-lactamase-producing Enterobacteriaceae in critically ill patients: Expected benefits and evidence-based controversies. Clin Infect Dis. 2019 May 30;68(12):2125-30. DOI: 10.1093/cid/ciy864
[11] Petersen RY, Hillman NH, Sadiq FH, Brownsworth CA, Williams HL, Josephsen JB. Effects of discontinuation of weekly surveillance testing on methicillin-resistant Staphylococcus aureus in the NICU. Am J Perinatol. 2024 May;41(S 01):e1337-43. DOI: 10.1055/s-0043-1763481

