Comparative evaluation of the aggregate index of systemic inflammation (AISI) and its modified version for early detection of central line-associated bloodstream infection: a pilot study using machine learning techniques
Gargee Anand 1Ketan Priyadarshi 2
Bandana Kumari 3
Jutang Babat Ain Tiewsoh 1
Rijhul Lahariya 4
1 Department of Microbiology, All India Institute of Medical Sciences, Patna, Bihar, India
2 Department of Microbiology, All India Institute of Medical Sciences, Deoghar, Jharkhand, India
3 Department of Biochemistry, All India Institute of Medical Sciences, Patna, Bihar, India
4 All India Institute of Medical Sciences, Patna, Bihar, India
Abstract
Background: Central line-associated bloodstream infections (CLABSI) are a common and serious problem in critically ill patients; their early detecting is challenging. This study evaluated the predictive ability of the aggregate index of systemic inflammation (AISI) and its modified form for early identification of CLABSI within two calendar days following central line insertion, using a machine learning approach.
Method: We conducted an analysis of patients who received central line insertion. Inflammatory indices were calculated using laboratory parameters obtained on second day post-insertion. Four machine learning algorithms were applied to evaluate their predictive performance for early CLABSI detection.
Results: Among 234 patients who met the inclusion criteria, 39 were confirmed CLABSI cases. We found both indices significantly elevated in the CLABSI group. Modified AISI demonstrated the strongest performance using XGBoost, with the highest area under the ROC curve (0.99), 97% sensitivity and 98% specificity, indicating its potential as the better early screening marker for CLABSI than AISI.
Conclusion: Both AISI and modified AISI demonstrated strong predictive value for early CLABSI detection, being both accessible and cost-effective. Modified AISI outperformed AISI in predictive performance. These findings support the need for the prospective validation of the modified AISI before clinical implementation.
Keywords
central line-associated bloodstream infection, CLABSI, aggregate index of systemic inflammation, AISI, early prediction, machine learning
Introduction
Healthcare-associated infections (HAIs), particularly central line-associated bloodstream infections (CLABSIs) are particularly concerning due to their rapid progression and high impact on patient outcomes [1], [2]. CLABSIs are associated with extended intensive care unit (ICU) stays, increased morbidity and mortality and significant financial costs to health systems globally [3], [4]. These infections can escalate swiftly to severe complications such as sepsis or multi-organ dysfunction, emphasizing the critical need for timely diagnosis [5]. Blood cultures are currently the cornerstone for diagnosing bloodstream infections [6]. However, their clinical utility is constrained by delayed processing times and limited sensitivity in early infection phases. Such limitations may lead to overtreatment and contribute to antimicrobial resistance [6], [7]. Therefore, identifying rapid, accurate and cost-effective biomarkers for early CLABSI detection remains a vital unmet clinical need.
Systemic inflammatory markers from routine blood tests, particularly the complete blood count (CBC) and the systemic inflammatory response index (SIRI), are increasingly studied as early indicators of infection [8], [9]. Ratios like the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have shown promise in various infections but are not well established for early CLABSI detection [10], [11], [12]. After central venous catheter (CVC) insertion, local injury to the vessel wall triggers a systemic immune response [13]. Neutrophils increase due to delayed cell death driven by inflammatory signals, while lymphocyte levels drop as part of stress-related immune suppression [14], [15]. Monocytes temporarily leave the bloodstream to enter tissues and aid in the immune response [16]. Platelets are activated by bacterial toxins and release cytokines that further drive inflammation [17]. In addition, albumin levels fall during inflammation due to reduced production and increased leakage from blood vessels [18]. As a negative acute-phase protein, albumin reflects both the severity of inflammation and the patient’s nutritional status [19].
These immune-hematological shifts underpin the rationale for composite indices such as the aggregate index of systemic inflammation (AISI), which incorporates neutrophil, monocyte and platelet counts relative to lymphocytes to reflect the host's inflammatory state [20]. While AISI has demonstrated prognostic utility in sepsis, cardiovascular disease and malignancy, its role in early detection of CLABSIs remains uninvestigated. Recognizing that hypoalbuminemia is a common and clinically significant marker of systemic inflammation and poor prognosis in critically ill patients, we propose a modified version of AISI, calculated by dividing the traditional AISI by serum albumin, to enhance its sensitivity and specificity.
Given that both CBC and albumin levels are routinely available within hours of ICU admission, this study aims to evaluate and compare the predictive performance of AISI and modified AISI for early CLABSI detection within two calendar days of central line insertion.
Materials and methods
Patient selection and data collection
This observational study was conducted among adult patients admitted to the ICU. From a total of 850 patients aged over 18 years who had a CVC placed in 2024, a statistically adequate sample size of 260 was calculated using the Taro Yamane formula, assuming a 5% margin of error and a 95% confidence level. The study population included all ICU patients aged 18 years or older who had a central line in place for more than two consecutive calendar days. Patients who presented with documented bloodstream infections at the time of admission were excluded. Case identification and infection surveillance were conducted in accordance with the standardized criteria of the Centers for Disease Control and Prevention’s National Healthcare Safety Network (NHSN) [21]. All patient information was anonymized before analysis by removing any identifying details.
Basic demographic variables (age and sex) and a vital clinical measure (body temperature) were recorded on the second day after central line insertion, along with blood-based inflammatory indices. These variables were chosen for their routine clinical availability, relevance to systemic inflammatory processes and low variability in measurement. Collecting only essential and easily available data makes this study practical and suitable for use in resource-limited settings, where access to advanced tests may be limited. We excluded other procedural confounders (catheter site and duration) due to low event rates, adhering to the events-per-variable (EPV) rule to prevent overfitting. Our analysis prioritized early CBC-derived inflammatory indices to reduce bias and ensure applicability in resource-limited settings. The calculation of inflammatory indices based on CBC included the following (20):
AISI: neutrophils (%) × platelets (thousands/microlitre) × monocytes (%) / lymphocytes (%)
Modified AISI: AISI / albumin (gram/decilitre)
Statistical analysis
Data was analyzed using SPSS version 26. The Shapiro-Wilk test was used to check if continuous variables followed a normal distribution. Variables were expressed as mean ± standard deviation (SD) when normally distributed and as median with interquartile range (IQR) when not. Categorical variables were summarized as counts and percentages. Patients were divided into two groups, CLABSI-positive and CLABSI-negative, and comparisons between them were made using the Independent t-test or Mann-Whitney U test for continuous variables, based on normality and the Chi-square test for categorical data. Relationships between inflammatory indices and continuous clinical variables were examined using either Pearson’s or Spearman’s correlation, depending on data distribution. Multicollinearity among predictors was checked using the Variance Inflation Factor (VIF). A p-value of ≤0.05 was considered statistically significant and marked with an asterisk (*).
To evaluate the predictive capability of CBC-derived indices—AISI and modified AISI—machine learning (ML) models were developed to predict the occurrence of CLABSI. Four primary models were developed: Logistic Regression, eXtreme Gradient Boosting (XGBoost), Support Vector Machines (SVM) and Adaptive Boosting (AdaBoost), using these indices along with key clinical variables (age, sex, and temperature) as input features. The dataset was split into a 70:30 training-to-test ratio to ensure proper evaluation. Each model's performance was assessed using standard classification metrics, including accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) with their 95% confidence interval. The area under the receiver operating characteristic curve (AUROC) was calculated to evaluate the discriminative ability of each model. All the ML algorithms were written in the Python scripting language (version 3.10.12, Python Software Foundation, Wilmington, DE, USA). Various libraries were used to create plots, ML algorithms, for data handling and numerical operations (Figure 1 [Fig. 1]).
Figure 1: Summarising the methodology and the clinical workflow of the findings of this study.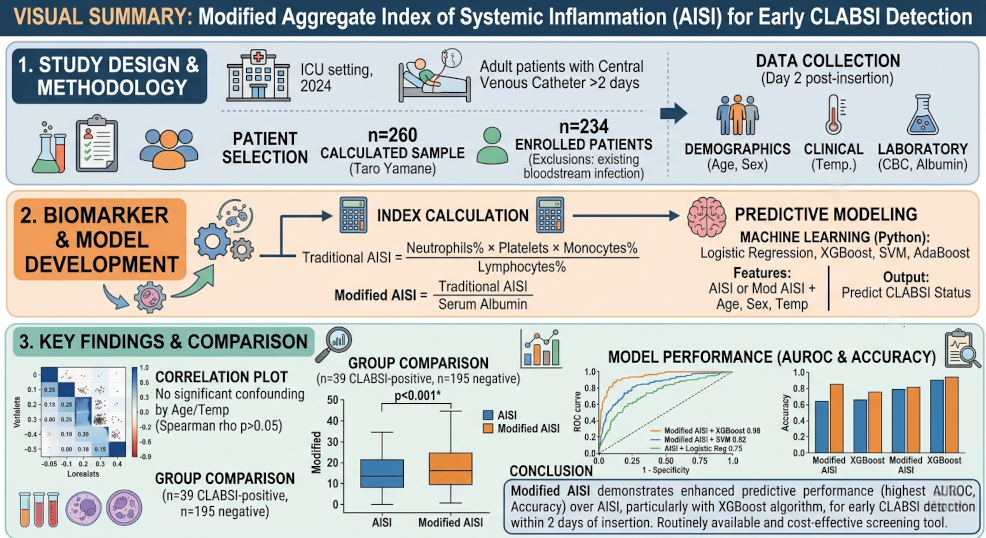
Results
A total of 234 patients were enrolled in the study, meeting the inclusion criteria. The median age of the cohort was 55 years (IQR: 41.3–67.0), with a higher proportion of male patients (58.5%). A comparative analysis of clinical and laboratory variables between CLABSI-positive and CLABSI-negative patients was performed and the baseline characteristics of the cohort are summarized in Table 1 [Tab. 1]. In the CLABSI-positive group, the median age was 55 years (IQR, 39.5–65), while the median age in the CLABSI-negative group was 56 years (IQR, 42.5–68).
Table 1: Demographic, clinical and inflammatory indices among CLABSI-positive and negative patients (N=234).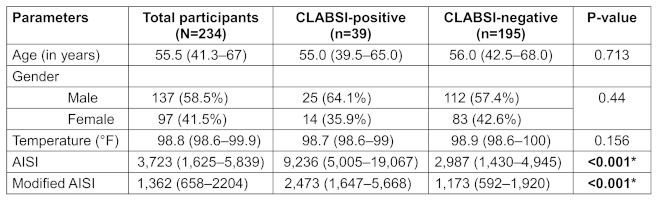
While age, sex and temperature did not show significant differences between the CLABSI-positive and negative groups, the inflammatory indices, including AISI and the modified AISI, demonstrated notable variations. These indices combine multiple immune cell values, allowing them to capture subtle changes that might not be apparent when assessing individual cell types in isolation. This integrated approach provides a more sensitive and comprehensive view of the body's early immune response to infection, especially with the introduction of the modified AISI. Prior to building model, we first examined the potential confounding effects of age and temperature on the inflammatory indices. This was done by assessing their correlations with each index using the Spearman rank correlation test. The results showed no significant correlations, suggesting that age and temperature were not strongly associated with the inflammatory indices (Figure 2 [Fig. 2]).
Figure 2: Correlation coefficient of the variables assessing the confounder.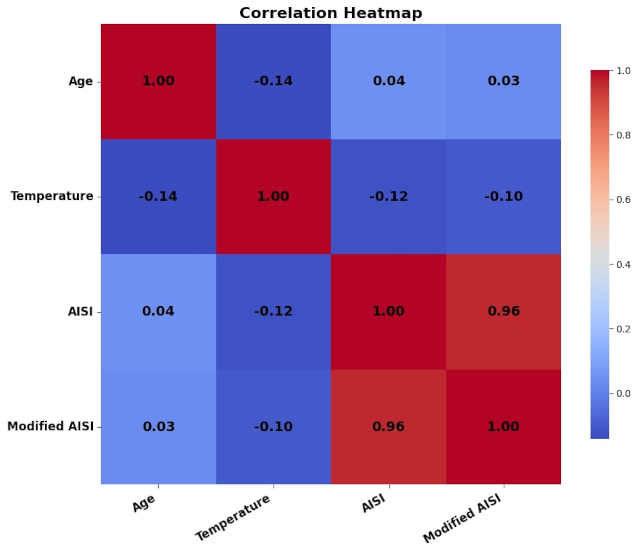
We further checked for the predictive power of AISI and modified AISI for CLABSI using four different ML algorithms, with the CLABSI-negative group set as the reference. Additionally, we assessed performance using several metrics, including accuracy, sensitivity, specificity, PPV, NPV and AUROC, which revealed distinct differences in the performance of the models for AISI and modified AISI (Table 2 [Tab. 2]). To mitigate potential biases arising from the relatively small sample size, bootstrapping was performed to resample the dataset and enhance the stability and generalizability of the model performance metrics. For AISI, logistic regression demonstrated a relatively lower performance, with high sensitivity but lower specificity and accuracy. In contrast, models like XGBoost and SVM showed much higher performance, especially in terms of accuracy, with high sensitivity and specificity, making them more reliable in distinguishing between positive and negative outcomes.
Table 2: Performance metrics of AISI and modified AISI in predicting CLABSI using various machine learning algorithms.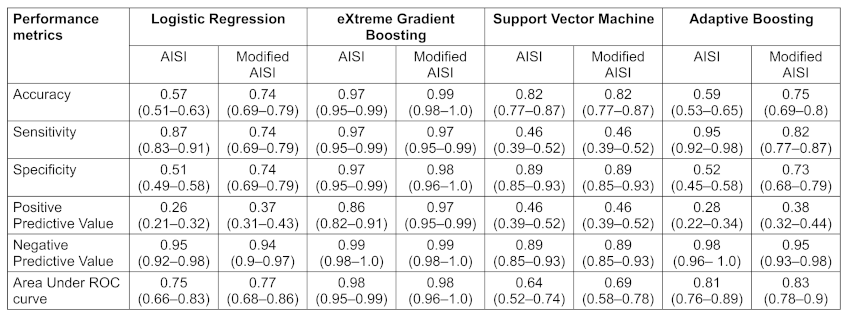
For modified AISI, both XGBoost and SVM maintained excellent performance, with accuracy near 100%, indicating their robustness in predicting the outcomes. Logistic regression and AdaBoost showed moderate improvements in modified AISI but were still less efficient compared to the other models. In summary, while modified AISI generally enhanced model performance, XGBoost and SVM consistently outperformed other models in both scenarios. In all cases, modified AISI's enhanced predictive power made it a more reliable and effective marker, underscoring its potential as a more robust biomarker for the early detection of CLABSI compared to AISI. Figure 3 [Fig. 3] and Figure 4 [Fig. 4] shows the comparative ROC curves of various ML algorithms for AISI and modified AISI, respectively.
Figure 3: Receiver Operating Characteristic curves comparing the diagnostic performance of AISI among various ML algorithms.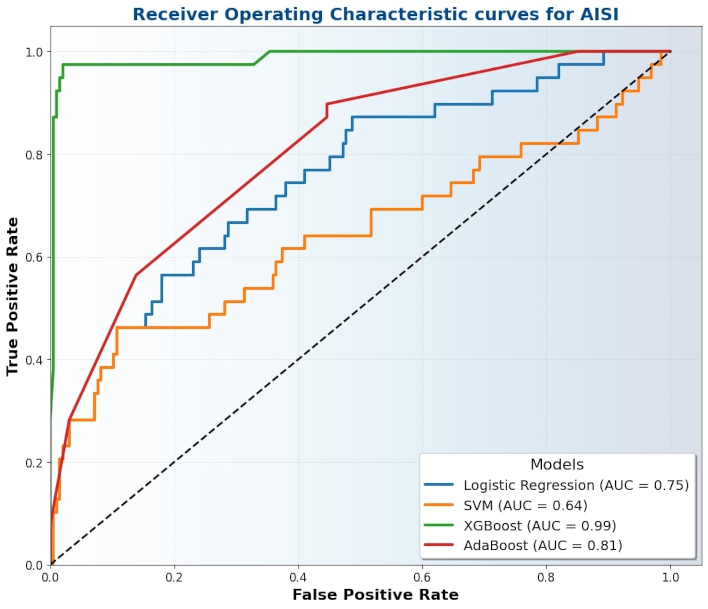
Figure 4: Receiver Operating Characteristic curves comparing the diagnostic performance of modified AISI among various ML algorithms.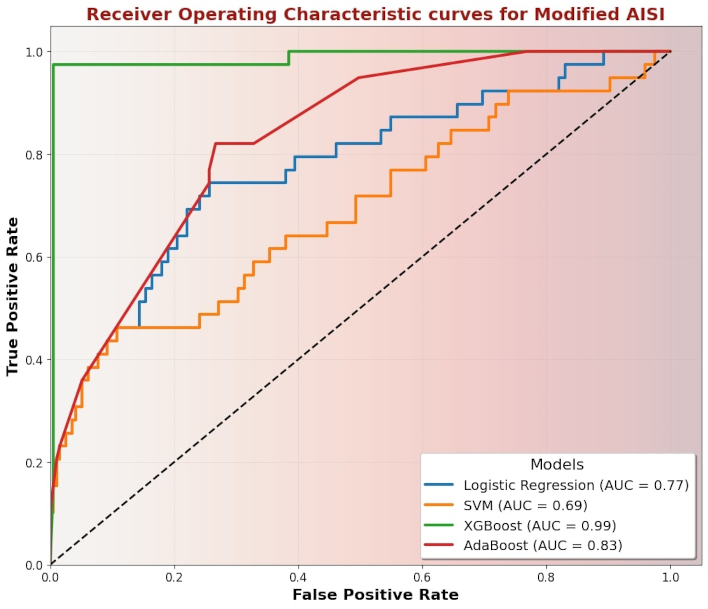
Discussion
CLABSI remain a significant cause of morbidity and prolonged hospitalization in critically ill patients, highlighting the need for reliable early detection methods [1]. CLABSI demand the most urgent attention than other HAIs, as it carries a burden comparable to the eighth leading cause of death in the United States [22]. Traditional diagnostic approaches, which often rely on clinical suspicion and basic blood parameters, can fail to identify subtle immune changes during the early stages of infection [6]. This study examined the use of composite inflammatory indices, AISI and modified AISI, which integrate multiple immune cell counts to improve detection. While age, sex and temperature showed no significant differences between CLABSI-positive and negative groups, both AISI and modified AISI exhibited substantial differences, with modified AISI demonstrating a stronger performance. Machine learning models, particularly XGBoost (0.99) and SVM (0.82), showed superior predictive accuracy with modified AISI as compared to Logistic Regression (0.74) and AdaBoost (0.75), indicating its enhanced potential for early CLABSI detection.
The insertion of a CVC causes a disruption in the endothelial lining, triggering a localized inflammatory response that increases the risk of infection [13]. This breach allows for the attachment of pathogens to the catheter surface and the formation of biofilms [23]. In response, the innate immune system activates rapidly: neutrophils are recruited as the first line of defense, releasing reactive oxygen species (ROS), enzymes, and forming neutrophil extracellular traps (NETs) to contain the spread of infection [24]. Monocytes are also attracted to the site, differentiating into macrophages that secrete pro-inflammatory cytokines [25]. Platelets are activated simultaneously, adhering to the damaged blood vessel and pathogens, releasing mediators that enhance immune cell recruitment and promote clot formation [26]. Endothelial cells upregulate adhesion molecules to facilitate leukocyte trafficking, while lymphocyte activity may be modulated, often showing transient depletion or redistribution as part of the systemic stress response [27].
AISI integrate various immune cell counts to provide a more comprehensive view of the immune status [28]. The modified AISI index further strengthens this approach by incorporating albumin levels, a key biomarker that reflects the body's nutritional status and inflammatory response. Albumin, being an acute-phase protein, decreases in response to inflammation, making it a useful addition to inflammatory indices [18]. The integration of albumin with immune cell counts in the modified AISI allows for a more robust and nuanced measure of immune response, potentially improving the early detection of infections. Machine learning models applied to these indices, such as XGBoost and SVM, can further enhance predictive accuracy.
In several studies, AISI has shown strong potential as a prognostic indicator across various inflammatory and infectious conditions, including odontogenic abscesses, COVID-19, sepsis and hypertension [20], [28], [29], [30], [31]. Studies demonstrate its superior predictive accuracy for disease severity and mortality compared to traditional markers like CRP or individual leukocyte ratios [29],[30]. Although very few studies have specifically evaluated AISI in CLABSI, its consistent performance in related systemic infections suggests promise for early detection and risk stratification in CLABSI [9], [32]. Incorporating albumin into the modified AISI may further enhance its sensitivity to inflammation and machine learning models can refine its predictive utility in clinical settings. As the NHSN defines CLABSI as a surveillance term, these biomarkers should be used only for case classification and not to guide antimicrobial therapy. Treatment decisions should be based on both clinical and microbiological assessments. We only looked at results from the first two calendar days after insertion, so using this test beyond this period would require further study with repeated measurements.
To the best of our knowledge, this is the first study to explore both AISI and modified AISI in the context of CLABSI. By incorporating ML algorithms for better evaluation, this study provided new insights about these accessible and hematology-based biomarkers for early detection, within 2 calendar days of central line insertion. These readily available and cost-effective markers could facilitate timely interventions, but there are certain limitations. First, the retrospective nature of data collection introduces selection bias, which may affect the predictive performance. Second, the small sample size of a single center, primarily due to our eligibility criteria and our centre’s relatively low prevalence of CLABSI. Despite this, the final sample has enough power for preliminary statistical analyses, may slightly impact the generalizability of the findings. Future studies should also assess whether using AISI and modified AISI to detect CLABSI early, can improve patient outcomes, such as reducing ICU stay or avoiding unnecessary antibiotics, to understand their true value in clinical practice.
Conclusion
This study highlights that inflammatory index, especially AISI and its modified version, can be useful for early detection of CLABSI within two calendar days after central line insertion. Both indices showed good predictive ability using the XGBoost algorithm, but the modified AISI had the best performance, with the highest AUROC, accuracy, sensitivity and specificity. These indices are based on routine blood tests and easy to calculate, making them practical tools for early screening and triaging. Further large-scale prospective studies are needed to confirm these findings and to explore their usefulness in different clinical settings and patient populations.
Notes
Authors’ ORCIDs
- Anand G: https://orcid.org/0009-0008-0473-389X
- Priyadarshi K: https://orcid.org/0000-0003-4623-3523
- Kumari B: https://orcid.org/0000-0001-5395-413X
- Tiewsoh JBA: https://orcid.org/0000-0003-0782-6588
- Lahariya R: https://orcid.org/0009-0003-5769-4509
Ethical approval
The study was approved by the Institutional Ethics Committee of All India Institute of Medical Sciences, Patna.
Funding
None.
Acknowledgements
We acknowledge the contributions of all authors to the conception, drafting, and critical revision of this original article.
Authors contribution
Ketan Priyadarshi, Gargee Anand and Rijhul Lahariya contributed to the conception and design of this manuscript. Rijhul Lahariya, Gargee Anand and Ketan Priyadarshi were responsible for the methodology and initial draft preparation. Literature search and data collection were conducted by Rijhul Lahariya, Bandana Kumari, Jutang Babat Ain Tiewsoh and Gargee Anand. The final draft was written by Rijhul Lahariya, Gargee Anand and Ketan Priyadarshi. All authors reviewed, revised, and approved the final manuscript.
Anand G and Priyadarshi K contributed equally to this work.
Ethical approval
This study was approved by the Institutional Ethics Committee of All India Institute of Medical Sciences, Patna (Ref.No. AIIMS/Pat/IEC/UG-STS/MBBS 2021/ Dec24/15). The requirement for informed consent was waived by the committee. All data were anonymized to maintain patient confidentiality, and the study was conducted in accordance with the ethical standards of the Declaration of Helsinki.
Competing interests
The authors declare that they have no competing interests.
References
[1] Centers for Disease control and Prevention. Healthcare-Associated Infections (HAIs). Current HAI Progress Report. 2025 [cited 2025 May 9]. Available from: https://www.cdc.gov/healthcare-associated-infections/php/data/progress-report.html[2] Anand G, Lahariya R. Healthcare-associated infections. GMS Hyg Infect Control. 2025 Dec 5;20:Doc76. DOI: 10.3205/dgkh000605
[3] Mosquera JMA, Assis Reveiz JK, Barrera L, Liscano Y. Impact of Central Line-Associated Bloodstream Infections on Mortality and Hospital Stay in Adult Patients at a Tertiary Care Institution in Cali, Colombia, 2015-2018. J Clin Med. 2024 Sep 11;13(18):5376. DOI: 10.3390/jcm13185376
[4] Lahariya R, Anand G, Sarfraz A, Tiewsoh JBA, Kumar A. CLABpredICU---AI-driven risk prediction for CLABSI in intensive care units based on clinical and biochemical parameters. Am J Infect Control. 2025 Aug;53(8):875-880. DOI: 10.1016/j.ajic.2025.05.016
[5] Alshahrani KM, Alhuwaishel AZ, Alangari NM, Asiri MA, Al-Shahrani NA, Alasmari AA, Alzahrani OJ, Ayedh AY, Qitmah MM. Clinical Impacts and Risk Factors for Central Line-Associated Bloodstream Infection: A Systematic Review. Cureus. 2023 Jun 25;15(6):e40954. DOI: 10.7759/cureus.40954
[6] Iyer V, Castro D, Malla B, Panda B, Rabson AR, Horowitz G, Heger N, Gupta K, Singer A, Norwitz ER. Culture-independent identification of bloodstream infections from whole blood: prospective evaluation in specimens of known infection status. J Clin Microbiol. 2024 Mar 13;62(3):e0149823. DOI: 10.1128/jcm.01498-23
[7] Aiesh BM, Daraghmeh D, Abu-Shamleh N, Joudallah A, Sabateen A, Al Ramahi R. Blood culture contamination in a tertiary care hospital: a retrospective three-year study. BMC Infect Dis. 2023 Jul 4;23(1):448. DOI: 10.1186/s12879-023-08428-0
[8] Agnello L, Giglio RV, Bivona G, Scazzone C, Gambino CM, Iacona A, Ciaccio AM, Lo Sasso B, Ciaccio M. The Value of a Complete Blood Count (CBC) for Sepsis Diagnosis and Prognosis. Diagnostics (Basel). 2021 Oct 12;11(10):1881. DOI: 10.3390/diagnostics11101881
[9] Lahariya R, Anand G. Early detection of central line-associated bloodstream infection in intensive care unit patients using the systemic inflammatory response index (SIRI). GMS Hyg Infect Control. 2025 Dec 5;20:Doc77. DOI: 10.3205/dgkh000606
[10] Jain R, Gopal A, Pathak BK, Mohakuda SS, Tilak T, Singh AR. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio and Their Role as Predictors of Disease Severity of Coronavirus Disease 2019 (COVID-19). J Lab Physicians. 2021 Mar;13(1):58-63. DOI: 10.1055/s-0041-1723057
[11] Goda R, Sharma R, Borkar SA, Katiyar V, Narwal P, Ganeshkumar A, Mohapatra S, Suri A, Kapil A, Chandra PS, Kale SS. Frailty and Neutrophil Lymphocyte Ratio as Predictors of Mortality in Patients with Catheter-Associated Urinary Tract Infections or Central Line-Associated Bloodstream Infections in the Neurosurgical Intensive Care Unit: Insights from a Retrospective Study in a Developing Country. World Neurosurg. 2022 Jun;162:e187-e197. DOI: 10.1016/j.wneu.2022.02.115
[12] Qu J, Yuan HY, Huang Y, Qu Q, Ou-Yang ZB, Li GH, Zhu HH, Lu Q. Evaluation of neutrophil-lymphocyte ratio in predicting bloodstream infection. Biomark Med. 2019 Oct;13(15):1255-1261. DOI: 10.2217/bmm-2018-0253
[13] Kolikof J, Peterson K, Williams C, Baker AM. Central Venous Catheter Insertion. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 May 10]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557798/
[14] Filep JG, Ariel A. Neutrophil heterogeneity and fate in inflamed tissues: implications for the resolution of inflammation. Am J Physiol Cell Physiol. 2020 Sep 1;319(3):C510-C532. DOI: 10.1152/ajpcell.00181.2020
[15] Wang Z, Zhang W, Chen L, Lu X, Tu Y. Lymphopenia in sepsis: a narrative review. Crit Care. 2024 Sep 20;28(1):315. DOI: 10.1186/s13054-024-05099-4
[16] Charles A Janeway J, Travers P, Walport M, Shlomchik MJ. The components of the immune system. In: Immunobiology: The Immune System in Health and Disease. 5th ed. Garland Science; 2001 [cited 2025 May 10]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK27092/
[17] Dewitte A, Lepreux S, Villeneuve J, Rigothier C, Combe C, Ouattara A, Ripoche J. Blood platelets and sepsis pathophysiology: A new therapeutic prospect in critically [corrected] ill patients? Ann Intensive Care. 2017 Dec 1;7(1):115. DOI: 10.1186/s13613-017-0337-7
[18] Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: Pathogenesis and Clinical Significance. JPEN J Parenter Enteral Nutr. 2019 Feb;43(2):181-193. DOI: 10.1002/jpen.1451
[19] Bretschera C, Boesiger F, Kaegi-Braun N, Hersberger L, Lobo DN, Evans DC, Tribolet P, Gomes F, Hoess C, Pavlicek V, Bilz S, Sigrist S, Brändle M, Henzen C, Thomann R, Rutishauser J, Aujesky D, Rodondi N, Donzé J, Stanga Z, Mueller B, Schuetz P. Admission serum albumin concentrations and response to nutritional therapy in hospitalised patients at malnutrition risk: Secondary analysis of a randomised clinical trial. EClinicalMedicine. 2022 Feb 11;45:101301. DOI: 10.1016/j.eclinm.2022.101301
[20] Association of SII and AISI in patients with sepsis: A retrospective study. Medicine Science. 2025 Feb 28 [cited 2025 May 9]. Available from: https://medicinescience.org/article/9919
[21] Centers for Disease control and Prevention. Bloodstream infection event (Central Line-Associated Bloodstream Infection and non-central line-associated Bloodstream Infection). 2026 Jan [cited on 2026 Mar 22]. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf
[22] Anand G, Lahariya R, Priyadarshi K. The rise of WHO-priority pathogens in central line associated bloodstream infection: Challenging the AWaRe paradigm in critical care. World J Microbiol Biotechnol. 2026 Jan 23;42(2):55. DOI: 10.1007/s11274-026-04797-1
[23] Mishra A, Aggarwal A, Khan F. Medical Device-Associated Infections Caused by Biofilm-Forming Microbial Pathogens and Controlling Strategies. Antibiotics (Basel). 2024 Jul 4;13(7):623. DOI: 10.3390/antibiotics13070623
[24] DeLeo FR, Allen LH. Phagocytosis and neutrophil extracellular traps. Fac Rev. 2020 Dec 21;9:25. DOI: 10.12703/r/9-25
[25] Arango Duque G, Descoteaux A. Macrophage cytokines: involvement in immunity and infectious diseases. Front Immunol. 2014 Oct 7;5:491. DOI: 10.3389/fimmu.2014.00491
[26] Herter JM, Rossaint J, Zarbock A. Platelets in inflammation and immunity. J Thromb Haemost. 2014 Nov;12(11):1764-75. DOI: 10.1111/jth.12730
[27] Dhabhar FS, Malarkey WB, Neri E, McEwen BS. Stress-induced redistribution of immune cells--from barracks to boulevards to battlefields: a tale of three hormones--Curt Richter Award winner. Psychoneuroendocrinology. 2012 Sep;37(9):1345-68. DOI: 10.1016/j.psyneuen.2012.05.008
[28] Zinellu A, Paliogiannis P, Mangoni AA. Aggregate Index of Systemic Inflammation (AISI), Disease Severity, and Mortality in COVID-19: A Systematic Review and Meta-Analysis. J Clin Med. 2023 Jul 10;12(14):4584. DOI: 10.3390/jcm12144584
[29] Tarle M, Raguž M, Lukšić I. A Comparative Study of the Aggregate Index of Systemic Inflammation (AISI) and C-Reactive Protein (CRP) in Predicting Odontogenic Abscesses Severity: A Novel Approach to Assessing Immunoinflammatory Response. Diagnostics (Basel). 2024 Sep 28;14(19):2163. DOI: 10.3390/diagnostics14192163
[30] Hosseninia S, Ghobadi H, Garjani K, Hosseini SAH, Aslani MR. Aggregate index of systemic inflammation (AISI) in admission as a reliable predictor of mortality in COPD patients with COVID-19. BMC Pulm Med. 2023 Mar 31;23(1):107. DOI: 10.1186/s12890-023-02397-5
[31] Xiu J, Lin X, Chen Q, Yu P, Lu J, Yang Y, Chen W, Bao K, Wang J, Zhu J, Zhang X, Pan Y, Tu J, Chen K, Chen L. The aggregate index of systemic inflammation (AISI): a novel predictor for hypertension. Front Cardiovasc Med. 2023 May 17;10:1163900. DOI: 10.3389/fcvm.2023.1163900
[32] Anand G, Lahariya R, Sarfraz A, Tiewsoh JBA. Early screening of central line-associated bloodstream infections: A novel comparative analysis of AISI, SII, and SIRI as predictive biomarkers. Am J Infect Control. 2025 Dec;53(12):1320-1324. DOI: 10.1016/j.ajic.2025.08.020

