Therapeutic factors of dance movement therapy from the perspective of patients and therapists – a multicenter clinical study
Laura Schwab 1Sophia M. Estel 2
Cornaro Clara 2
Amanda Freiberg 3
Andrea DuBois 4
Sabine C. Koch 1,2,5
1 School for Therapy Sciences, SRH Hochschule Heidelberg, Heidelberg, Germany
2 Research Institute of Creative Arts Therapies (RIArT), Alanus University for Arts and Social Sciences, Alfter, Germany
3 Clinical Creative Arts Therapies Department, Mediclin, Bliestal Kliniken, Blieskastel, Germany
4 DGD Klinik Hohe Mark, Oberursel (Taunus), Germany
5 Faculty of Fine Arts, Creative Arts Therapies Research Unit (CATRU), University of Melbourne, Australia
Abstract
There is growing evidence from clinical outcome studies that dance movement therapy (DMT) has multiple beneficial effects on health. Therefore the question of the therapeutic factors of DMT is currently gaining momentum: How does DMT bring about therapeutic change? In a multicenter clinical study, we assessed the therapeutic factors of DMT from the perspective of patients and therapists in eight psychosomatic and psychiatric clinics in Germany. The data sets of these experts by experience comprised the written responses of N=203 patients, which were subjected to a thematic analysis, and extended by the transcribed responses of N=6 therapists from a group interview. Results of the patient data suggest three clusters of therapeutic factors, regarding (1) the general conditions of the therapy sessions, designated as structure, (2) the self-exploration of the patients, with the most frequently coded sub-categories of (a) body awareness, (b) access to emotions and (c) expression of emotions, and (3) the self-management of the patients. DMT was highly accepted and appreciated by the patients as a central therapeutic source of their clinical treatment. Without having been asked for it in the survey, more than 10% of the patients stated a request for the expansion of DMT, especially in aftercare in the outpatient setting. The therapists emphasized active embodiment as one of the most important change factors and the self-efficacy boosting and action-based transfer-to-practice effects of DMT. A comparative analysis of the therapeutic factors in our sample with those previously reported, yielded a considerable fit with recent therapeutic factor models. The reliable observation of and assignment to factor dimensions provoked a critical method discussion regarding their definition and delimitation. The most frequently assigned therapeutic factor domain in the patient and therapist data was embodiment. While still a concept in need of clarification, the distinction into active and receptive components of embodiment helped to create some clarity of its domain scope and further delimitation
Keywords
dance movement therapy, therapeutic factors, clinical multicenter study, written survey, group interview, thematic analysis
1 Introduction
Research into the therapeutic factors of dance movement therapy (DMT), as well as into all creative arts therapies, is critical to the advancement in this field [1]. By better understanding how DMT interventions work, we can more appropriately tailor them to the needs of the clients and the specific goals of the therapy.
DMT works indirectly on cognition [2], directly on affect and emotions [3], on the reduction of depressed and anxious affect, and stress [3], [4], [5], [6], [7], [8], on pain reduction [9], as well as on the increase of well-being and quality of life, body image, interaction, and psychomotor aspects [7], [10], [9], [11], [12].
Moreover, DMT is part of the Creative Arts Therapies (CATs) together with music therapy, art therapy, drama therapy and poetry therapy [1]. The aesthetic experience (defined as the experience of beauty and authentic expression) may be a unique therapeutic factor of CATs and can occur through different arts media (dance, art, music, theatre). According to the model of embodied aesthetics from Koch [13], next to (a) aesthetics, other body-related holistic factor clusters are: (b) expression and communication through the body (symbol), (c) playfulness and pleasure (hedonism), (d) a protected/safe therapeutic space, where action and interpersonal interaction can be explored and rehearsed (enactive therapeutic space), and (e) the activation of strength, resources, self-efficacy beliefs and constructive action through experiencing creation, freedom, productivity and efficacy (generativity). De Witte et al. [1] investigated the therapeutic factors of the CATs in a scoping review of n=64 available empirical studies, and found 19 domains of therapeutic factors, with the three main unique factors across the CATs being (a) embodiment, (b) concretization, and (c) symbolic communication.
Since embodiment plays a pivotal role as a therapeutic factor, it is important to define it. The authors of this study rely on the following definition of embodiment: Embodiment denominates “bodily phenomena in which the body as a living organism, its movements and functions as well as the interaction of body and environment are assigned a central role in the explanation of and interaction with thinking, perception, learning, memory, intelligence, problem solving, affect, attitudes and behavior” [14]. Fuchs [15] uses the German term “Leiblichkeit” (corporeality) to describe the living body and its relationship to the world via resonance through its own senses [16]. The concept of bidirectionality specifies the reciprocal interaction of emotional expression and affect impression: state of mind and affect are not only expressed through movement, but movement also affects state of mind and affect [13], [17]. Bodily resonance, as any kind of local and overarching sensation of the body, is a medium for emotions, states of mind and attributions of meaning; changes in bodily resonance have an influence on affect and perception [3], [13], [14], [18], [19], [20], [21], [22], [23]. The consistency of definitions of embodiment between different authors does not always seem to be given [24], as picked up in the method-critical part of the discussion.
In our study, we explored the question of therapeutic factors from a participatory perspective focusing on what the patients experience to be effective in DMT, how they describe that DMT works for them, and the needs and wishes that result thereof. The patient perspective is complemented by that of the therapist, encompassing their own comprehension of how DMT works and the perceptions and feedback they received from their patients. As an exploratory analysis, we matched Koch’s model of embodied aesthetics [13] and the findings of De Witte et al. [1] with the resulting therapeutic factors of DMT. In this article we use the term ‘therapeutic factor’ and ‘change factor’ interchangeably. While both terms bring forward the quality of change experienced behind the factor, we use therapeutic factor more frequently as it brings forward the therapeutic context - which is in essence a context of change. In the process of gathering data from patients and therapists we did not use these technical terms but stayed with asking how and why questions.
The present study is a continuation of the study by Estel and Koch [25], which used mixed methods to investigate the change factors of DMT in a clinical setting under naturalistic conditions. Next to open questions, which provide the data for this study, it also included scales on specific factors of DMT (DMT-SF; [26]), joint factors of CATs (AF-CATs [23]), and common factors of psychotherapy (FEPiG 44 [26]) which are not part of our analysis here (for quantitative analysis see [25]). In this article, we expanded on the qualitative analysis, and investigated how patients themselves and their therapists, as experts by experience explained the effects of DMT in their own words. We have made a distinction between expert by (a) first person experience (here the patient affected by the mental health condition) and (b) second person experience (here the therapist, expert by training, and experiencing the process of therapy and the helpful elements/therapeutic factors with the patient). The therapists, as experts involved in the therapeutic process, were consulted as a further valuable source of information in relation to the object of research. We asked the following research question: What are the therapeutic factors of DMT for the patients and their therapists?
2 Methods
In a written survey conducted over the duration of two years, N=203 patients answered four open and item-based questions in a therapeutic factors’ questionnaire at the end of their treatment yielding N=748 patients’ responses (arising from patients multiplied with four items without unanswered/empty answer fields). Before completing the scales (quantitative part as described above; [25]) patients freely wrote down how DMT worked for them. The resulting response sequences are the basis of our analysis in this paper. The assessment of the patients’ free text responses was carried out with a thematic analysis (TA) [27], [28], [29]. The TA provides the diversity and scope of the subjective impressions of the answers and presents them in thematic networks with different hierarchical levels of abstraction [27], [28], [29].
In addition, six therapists (N=6) involved in the study were interviewed about the effectiveness of DMT. The inclusion of the therapists’ perspective is another way to examine the research question. As those who hold the space and are likewise involved through their accompanying of the therapeutic process, the therapists are a valuable target group for a survey on therapeutic change factors. Their statements were transcribed and analyzed by a qualitative synthesis.
2.1 Study design and sample
A one-group-pretest-posttest design was implemented in eight German psychotherapeutic or psychosomatic clinics, each with inpatient and/or outpatient settings with DMT as part of an interdisciplinary, multimodal treatment approach. The participating eight dance movement therapists (N=8) – each working in one of the clinics – were recruited via the Berufsverband der TanztherapeutInnen Deutschlands (BTD) [30]. They were all certified DMTs, seven had been trained at recognized institutes of the BTD, one had been trained at another institute. They had responded to a call for participation via the professional association email-listserv and worked with patients from their own clinical institutions. Patients were assigned to the DMT groups based on the general treatment plan of their clinics and participated voluntarily in the study.
The general conditions of the clinics (range of settings, therapy forms and their orientation) differed, as did the frequency and duration of the DMT units (45 to 120 min). There was also heterogeneity regarding the patients’ diagnoses and, consequently, the specificity of the therapeutic objectives. Accordingly, the therapists adapted their approach and focused on the circumstances and needs of their patients and relied on different approaches and procedures in a process-oriented manner. As a general structure, the sessions consisted of an initial part with a verbal well-being round and/or physical warm-up exercises, a main part with a topic-specific and/or movement-specific focus and a verbal exchange and/or a conclusion in movement (for a tabular overview, see [31]). Examples for concrete content in partner work included hand or foot dialogs, partner-based mirroring in different rhythms and movement qualities, working with the 5 rhythms according to Roth [32] and psychoeducational elements such as introduction of the body-mind-spirit concept [31]). The total samples were composed as follows in Table 1 [Tab. 1] and Table 2 [Tab. 2].
Table 1: Characteristics of sample of patients participating in the study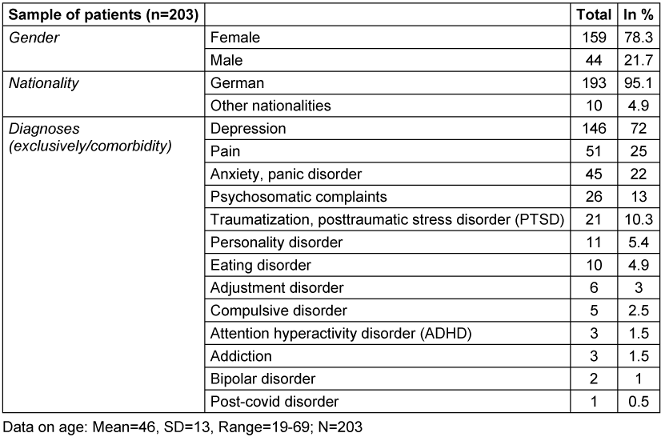
Table 2: Characteristics of the sample of the patients’ therapists who were interviewed 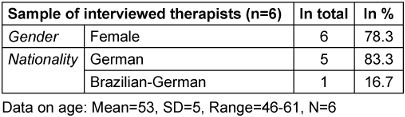
2.2 Instruments and data analysis
2.2.1 Instruments and data analysis for the sample of patients
The qualitative data informing this article, was collected exclusively in the final questionnaire of the post-test’s questionnaire catalog. The final questionnaire was completed by the participating patients in paper form or online after the end of their therapeutic treatment. At the beginning of this questionnaire, before the standardized scales, patients were asked to reflect on their therapeutic process. The first item was embedded in the analysis of the three types of therapy which the patients perceived as most helpful among the multidisciplinary treatment in their institution. They were asked to identify these three most helpful methods, followed by the question (the questionnaire was written in German, the questions were translated into English for the article by the first author):
- How exactly did these 3 forms of therapy help you?
If DMT was described as one of the three most helpful forms of therapy, the according answer was coded.
Subsequently all participants were requested to respond to three open-ended questions, in which they were asked to retrospectively describe in their own words how and why DMT had worked for them. They were listed in the questionnaire under the heading: ‘Questions about dance/movement therapy treatment’:
- Please summarize in one sentence HOW dance therapy, has helped you. ("Dance movement Therapy has helped me in that ...”). [Capital letter as in the original questionnaire]
- Was there an EXPERIENCE in the process of dance therapy that was particularly helpful or healing for dealing with your problems? If so, please describe this experience and how you believe it came about.
- Was there a single EXERCISE in dance therapy that was particularly enriching for you? Please name this exercise and describe why this was particularly enriching for you.
The patients’ answers to these four questions were analyzed with thematic analysis [27], [28], [29]: In six rule-guided steps, patterns of meaning – so-called themes – were identified and indexed in the data set (manually and using the text interpretation software MAXQDA2022). The free text responses were examined for common patterns with regard to the mode of action of DMT. This resulted in the Basic themes (BTs) at the first level. These were often formed as In-Vivo-Codes, i.e. from the verbatim formulation or designation of the patients. Individual statements were assigned to different BTs where appropriate. Based on similarities and overlaps between the codes, they were systematized into higher-level Organizing themes (OTs). Clusters of therapeutic factors were then assigned via the OTs as Global themes (GTs). Two female raters (German DMT students, 38 and 52 years old), both White, with the first author of this study rating the complete data and a second rater (not part of the author team), trained in the coding scheme, rating 5% of the data, showed an agreement of 80%, with Cohen’s Kappa κ=0.7, p=.000. Subsequently the BTs were adjusted to the existing theoretical model of Koch [13] and empirical derived categories of De Witte et al. [1] (see discussion 4.3).
The open feedback section at the end of the patient questionnaire contained the concluding item: "If you have any comments on this questionnaire or this study, we look forward to receiving your feedback", which was heuristically analyzed by a mixed quantitative and qualitative synthesis of the first author (a White woman of 38 years).
2.2.2 Instruments and data analysis for the sample of interviewed therapists
On the therapist side, a group interview was conducted by the second author on 19 January 2021 as part of an online video conference with six dance movement therapists who were involved in the study to organize their data collection. The interview focused on the therapists’ perspective on the therapeutic factors experienced by the patients. Therapists were asked:
- What makes DMT effective in your (therapists’) view, and
- What feedback do you receive from the patients about how DMT works for them?
The group interview lasted 45 minutes and was subsequently transcribed. The statements were analyzed by a qualitative synthesis of the second author SE (a White woman of 30 years) and double-rated by the third author CC. The analysis revealed that some statements of the therapists contained more than one description of examples or situations relating to the same therapeutic factor; in the analysis the data was split into coding units to label and assign them to the theory model and the empirically derived domains of therapeutic factors – thus the higher the number of assignments the more emphasis on that specific cluster or category by the therapists. The agreement of SE and CC regarding the categorization of the units to be coded was 85.71% with Cohen’s Kappa κ=0.783, p=.000. The assignment of these to Koch’s model [13] resulted in a match of 46.43% with Cohen’s Kappa κ=–0.053, p=0.627 and in the 19 domains of De Witte et al. [1] of 66.67% with Cohen’s Kappa κ=0.524, p=.000 with at least one match for multiple assignments. We did an additional exploration on how these results and the therapeutic factors categorized here tie back into the theory [13] and empirical derived categories of De Witte et al. [1] (see discussion 4.3).
As a final exploratory step, a comparison of the BTs from the patients’ data and therapists’ coded statements was conducted with the use of the theoretical clusters of therapeutic factors of art therapies by Koch [13], and the empirically found therapeutic factors conceptualized in the 19 domains by De Witte and colleagues [1] – on the one hand to generate comparable categories for the patients’ and therapists’ data and on the other hand to connect our findings to previous research. The data was analyzed in an explorative heuristic way by first, second, third and last author (LS, SE, CC, SK) whereby the patient’s data was analyzed on the level of the Basic themes (BTs) raised by the thematic networks and the therapist’s data on the level of single statements made in the group interview mentioned above. The coded units were assigned to the clusters and categories of the two models; mentions were counted in total, and the percentage share of the total result was calculated (see 3.4.1 and 3.4.2). Multiple assignments were permitted.
Figure 1 [Fig. 1] shows an overview of data and methods used that inform this article.
Figure 1: Overview of study content and methodology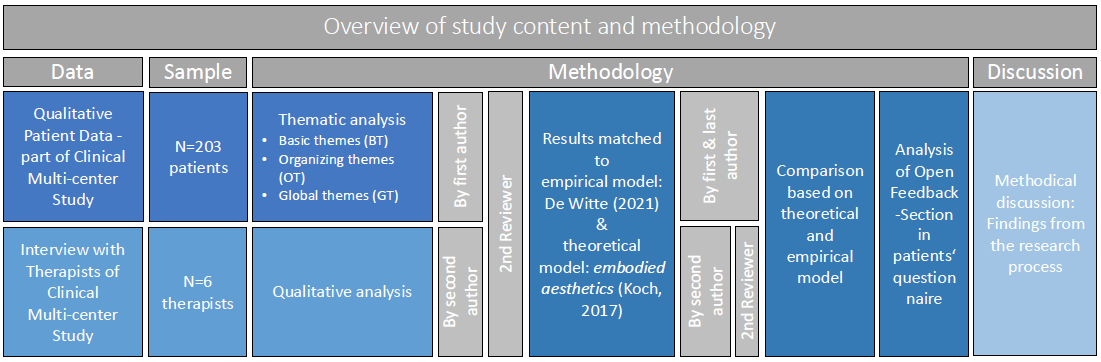
All data was collected and analyzed in German. The translation into English for this article was carried out with the help of the translation program DeepL 24.2 (free online version).
3 Results
3.1 Thematic analysis and networks on therapeutic factors of DMT from patients’ perspective
The following section presents the three exploratory thematic networks (TNs) derived from the thematic analysis of the four above-mentioned open questions answered by the patients on the therapeutic factors of DMT. These networks are presented in condensed form, with illustrative examples from the data integrated throughout. For examples of coded patient statements for each individual Basic Theme, see Attachment 1 [Att. 1] (German). The resulting TN consist of the three Global themes (GTs): (1) Structure (Figure 2 [Fig. 2]), (2) Self-exploration (Figure 3 [Fig. 3]) and (3) Self-management (Figure 4 [Fig. 4]).
Figure 2: Thematic network Structure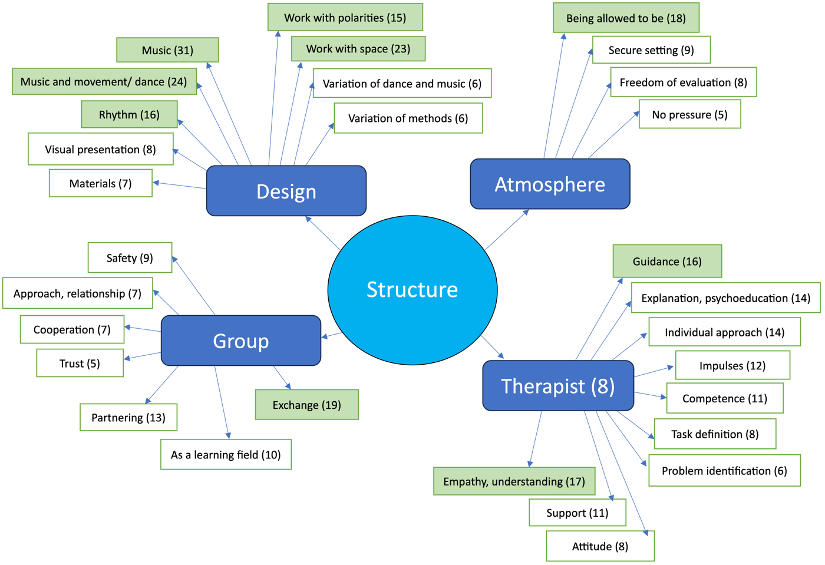
Figure 3: Thematic Network Self-exploration
Figure 4: Thematic Network Self-management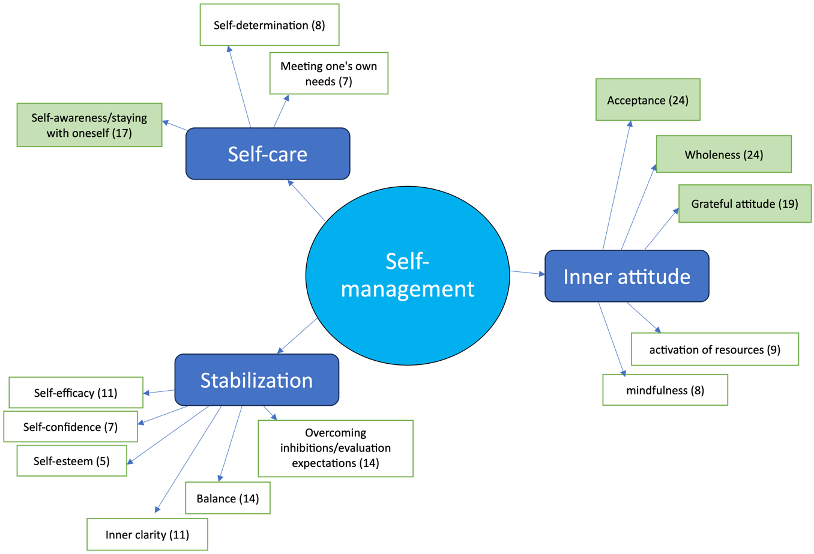
(1) Global theme (GT) Structure: In more than 364 codes – divided into four OTs – the patients described the therapeutic factors that were initiated externally or outside of themselves within the DMT sessions. The Organizing theme (OT) Design (n=136) subsumes the codes that included predetermined creative elements. 31 times the patients named the Basic theme (BT) Music without further context, often as a key point, and 24 times in connection with Movement and/or dance, as in the statement of ETGG19 (ETGG19 represents an anonymized designation of a patient): “By translating music into movement, I had more access to my creativity”. “Through the music, this rhythm, I felt connected to myself and the whole world”, stated the same person as one of 16 examples for the In-Vivo-BT Rhythm. 15 patients’ statements included the Work with polarities (BT), as exemplified in the utterance by PDHG15: “Perceiving extremes in me - through an exercise in which I made extremely fast and extremely slow movements.” The BT Work with space emerged 23 times, for example in ETCE03s description of the realization through a helpful DMT exercise: “How big my own space is around me, namely very small.” The OT Atmosphere was most clearly determined by the BT Being allowed to be with 22 codes. In this BT, the patients described the experience of being allowed to show themselves authentically without having to hold back or pretend, as KEBE24 expresses with the words: "[...] and could be completely myself [...]”. Other BTs regarding Atmosphere (OT) are, for example, a Secure setting with nine codes. In the OT Group, coded 71 times, the BT Exchange dominated with 19 codes - alongside the BT Safety with nine codes, Partnering with 13 codes and the group As a learning field with 10 codes. SGRE21 described Exchange (BT) as follows: “Conversations and exchange with rehabilitants in the group as well as feedback from the therapist” and with this sentence also refers to the last OT Therapist, under the GT Structure with a total of 117 codes. This includes the BT Guidance (n=16) with statements such as from PADG17: "Dance therapist who brought out deeply hidden (“buried”) emotions in me through dance and music. Super!”. The BT Explanation, psychoeducation indicates that the therapist’s explanatory words in the DMT were effective. The BT Individual approach includes responses in which the patients describe how the therapist responds to the individual patients: "Trust in the therapist, who responded to the patients very individually and with a wide variety of methods” (ORFE20); the latter two BTs were coded 14 times each. In addition, the patients’ statements often literally pointed out to the BT Empathy, understanding of the therapist (In-Vivo-Coding) 17 times.
(2) GT Self-exploration: The most comprehensive of the three GTs comprises 983 codes – including the three BTs with the highest absolute prevalence – and largely depicts processes that the patients experienced as effective. The OT Expression is about processes of expression with 101 encodings. The Expression of emotions (BT) is reflected in 55 codes, some of which were adopted In-Vivo, as in KEJH10: “Expression of emotions to music and in movement [...]”. Movement, body and dance as a means of expression form three further BTs with five to 15 codes. The above example from KEJH10 also includes Movement as a means of expression (BT). The patients’ articulation of the aspect of Perception (OT, n=314) constitutes the OT with the highest number of codes. This is also due to the fact that the most frequently occurring BT, Body awareness (n=72), and the second strongest BT, Access to emotions (n=63), are subordinate to this OT. HDBE03 combines both in the exemplary answer: "I got to the emotions through my body sensation.”The patients also mentioned nine to 28 times that they had experienced Access to their needs (BT), problems (BT), boundaries (BT) and the past (BT). Several times, statements about this also occurred in combination, as with FREE21: "I was able to determine my personal boundaries and recognize my needs” or, as described in more detail by HDIG07: "I learned to feel into my body, to notice what its needs are and what my emotional needs are [...]”. Patients also described or focused on the Actual state (BT, n=7), the Here & now (BT, n=8) and the undefined inner self (BT: Access to the inner, n=7). The last group of similar BT consists of the perception of moods: Many patients stated the experience of joy (n=24). Lightness (BT, n=13), an increase in Strength/energy (BT), a feeling of Well-being (BT) and a general Improvement in mood (BT) were also coded as individual BTs to be able to convey the effect of positive mood or positive affect in OT Perception more precisely. The OT Opening up with 69 codes includes processes of action that are related to patients opening themselves up to something, opening up to or about Creativity (BT, n=9) or Rediscovering (BT, n=23) something. The BT New experiences, New access, Self-opening and Engaging in therapy with 5 to 18 codes also form it. An example of the coding of the BT Creativity from KEWE23 is: “Creativity – new possibilities to discover access to the subconscious.” Patients listed Relaxation (BT) as a helpful experience 20 times. Feeling free or liberated shows up 22 times in the data as an effective experience. HDDE01 also stated: "I trusted myself a lot more over the course of the therapy and felt like I was liberated.”, which led to the BT Freedom/liberation. Allowing emotions and Free movement/improvisation were coded as BTs 22 times; the latter in statements such as "The free dancing, I was able to let go of everything that was weighing me down." (ENBE13). The OT Letting go abstracts from this and similar descriptions by the patients that the process of letting go (of something) influenced them. Six additional BTs, which describe the outline of Distraction from pain (BT, n=5), from problems or mental and physical letting go, add up to a total of 65 codes. Some patients mentioned the term Movement (BT, n=26) in keywords or its use in various exercises an effective experience: "Release strong emotions through deep breathing in movement." (HTEE23). From the patients’ more explicit explanations, that procedures and processes – which otherwise take place on a different level – could be experienced using the body and/or that they were able to rehearse behavior in this way, the BT Physical experience/rehearsal of movement was developed (n=20). They often mentioned that they practiced Setting boundaries (BT, n=20). The explorative character common to the active processes led to the 103 times coded OT Exploration. HLKG21 wrote about the item after the question of how DMT works: "Impulses led to insights." The following topics or BTs resulted from similarly directed answers from this person and the other patients: Recognizing new insights/ connections (n=29), Insights into own patterns (n=23), Insights into new strategies for action (n=17), Self-knowledge (n=27). "DMT worked because I learned more about the connection between mind and body in different ways." (AEBG01), refers to Findings on the connection between body and psyche (BT), which was coded In-Vivo and led to a 17-fold BT, which, like all BTs under this OT, does not contain any duplicate mentions from the BT New insights/connections. Since the patients reported experiencing new insights in 140 segments, these were brought to the next higher level of abstraction as OT Comprehension. In the TA, the BT Principle of embodiment (n=9) is also shown under this OT. At this point it means learning about the mechanism of embodiment. From the fact that DMT worked for one person participating in the study in such a way that the person was able to "process fears" (KEHE20) and related statements, the systematization for the BT problem handling (n=15) emerged. With the BT Overcoming problems, consisting of 17 mentions of topics such as "handling acute problems" (CALE25), the BT Dealing with emotions (n=17) and the BT Dealing with boundaries (n=6) form the OT Handling (n=55). This OT includes processes of the patients that identify an active and productive confrontation a therapeutic factor of DMT. The OT Reflection (n=52), on the other hand, covers processes in which DMT works by patients integrating what they have experienced into their own thought constructs. This OT was superimposed on the BT Transfer to everyday life/own life (n=20), the BT Awareness (n=15), the BT Change of perspective and Self-reflection. Statements of patients experiencing that certain mechanisms, circumstances and behavioral patterns were effectively transferred from the subconscious to the conscious mind form the basis for the BT Awareness. HEARIA99 explains that" [...] I became aware that I am allowed to be who I am." All the OTs under the GT Self-exploration were labeled with terms that describe processes, i.e. in this context, processes of action. The underlying OTs can be grouped differently: on the one hand into active processes of different dimensions, such as the OT Body awareness and the OT Access to emotions (which expresses not only the perception of emotions, but also the aspect that perception, which was previously not possible, became possible) and on the other hand the OTs can be grouped into the different topics that were experienced through the respective process.
(3) GT Self-management. The third GT is based on a total of 176 codes and belongs to one of the two GTs that relate to the ‘inner’, that is the factors that change the person’s inner self, whereby the sub-themes of Self-management (GT) imply the development and strengthening of a positive attitude and a positive behavior towards oneself. It is formed from the first OT Inner attitude with 82 codes. 24 of these come from the BT Acceptance, which points out, when patients reported to be able to accept themselves, their body or circumstances, as LSKE11 puts it: "I learned to accept and love my body, because I only danced for myself." Patients also referred to the connection between body, soul and mind 24 times. The coding of Holistic approach (BT) took place if all three words occurred in one segment. The BT Grateful attitude occurred 19 times, mainly in connection with the fourth question about a helpful exercise of DMT with formulations as by ETRE23: "gratitude to the body [...]". The BT Mindfulness contains six codes and Activation of resources nine codes; the second OT Stabilization (n=62) with patients reporting 14 times that they achieved Balance (BT) and Overcoming inhibitions/evaluation expectations (BT). Patients often literally uttered the strengthening of Self-efficacy (BT), Self-confidence (BT) and an improvement in Self-esteem (BT) and the achievement of Inner clarity (BT) five to 11 times. The 32 codes of BTs listed under the OT Stabilization can regard outcome measures, i.e. effects of DMT. They arose from the question of the mode of action and at the same time depict it. "I can withdraw (from others) without being looked at crookedly" (ETWE18) is one of 17 statements on Self-awareness/staying with oneself and represents a BT of the last OT Self-care. The TN also depicts Self-determination (n=8) and meeting one’s own needs (n=7) as further BT.
The comparison with the theoretical clusters of Koch [13] shows that overall, the BTs of the TN (based on the statements of the patients) are almost even between active (n=70) and receptive aspects (n=75) of the therapeutic process. Frequent mentions on the receptive side relate to body awareness, a sense of resonance, safety, contact with oneself and flexibilization, and on the active side to emotional expression, explorative space, yielding (letting go), opening up to new experiences, and joyful aspects of moving.
3.2 Open feedback section of patient questionnaire
The results of the open feedback question of the patient questionnaire with 51 statements revealed three main themes: (a) their dance therapist was mentioned positively to very positively (n=11); (b) DMT was mentioned as useful and/or beneficial (n=15); and (c) the recommendation was made that DMT should be made accessible to all patients and/or the desire was expressed to have the opportunity to access an outpatient DMT service (n=24).
3.3 Therapists’ perspective on therapeutic factors of DMT
In the statements about how DMT works from the perspective of the therapists, the most frequently mentioned aspect was coming into contact with oneself; the latter included aspects such as self-exploration, self-perception, self-confidence, identity, and self-determination. One therapist described this for herself: "that I have the feeling that I am really coming to myself and to what I feel [...], I am coming to my will, to my wishes" - and in relation to her patients she says: "It is so great to see when people get to know themselves a little bit". This shows that, from the therapists’ perspective, DMT addressed various factors that were mentioned by the patients in the thematic networks Self-exploration and Self-management of this study.
According to the therapists, the effect of DMT is achieved by using physicality or the body as a resource. As one therapist puts it: "I trust the knowing body [...] the most [...], I learn from myself in movement". Another therapist shares the feedback that some patients say: "Dancing doesn’t work for me or I can’t - and when they have taken part in such a body work, they often say: ‘ohhha that worked’ or ‘I somehow feel much better now’ or ‚I feel light now’ or ‚I somehow feel liberated, I don’t even know from what’ - it’s often great as an introduction".
Another therapist shared the fact that DMT enables the transfer of experiences to other contexts through its body-based approach, saying: "This physical experience really comes back in everyday life and is linked, which makes it very action-orientated and very practical". She also quoted the feedback from a patient: "I understood a lot here [in the clinic], but through dance therapy it really came into my body and [I] was then able to put it into practice, so to speak". These statements refer to BT Physical experience/rehearsal of movement, and BT Transfer to everyday life/own life, mentioned by the patients, with the therapist’s perspective being confirmatory at this point.
Experimenting, researching and behavior in rehearsal (comparable to OT Exploration and its BT Physical experience/rehearsal of movement in the patients’ data) were the second most frequently mentioned responses from the therapists to our questions. They gave the following feedback on how the patients experienced DMT as effective: "Having new opportunities to act differently. In other words, the ability to act, to try things out". About the kinesphere (i.e. the space surrounding the body) another therapist said: "you can feel it very clearly. So, they have [...] a tightness in the movement. If they do well, they spread out more, take up more space and that is [...] from my side, but also as feedback, more mobility". Two other therapists also mentioned this aspect in terms of the ‘flexibilization’ (vs. rigidity) that would be possible within DMT, both physically and mentally.
"I think community is another important aspect of dance therapy. [...] I believe that this also happens because they really experience themselves so physically with each other, and not just on a cognitive level, not just in a discussion group, but really [...], they have moved together" is another therapist’s statement. This refers to the Connection with others, which is the third most frequently mentioned therapeutic factor of DMT by the therapists. Mirroring, being seen, changing perspective and empathy were reported as helpful by the patients. Regarding the Thematic Network Structure, the therapists’ statements here also coincide with those of the patients in the OT Group and its BTs (for full transcription see Attachment 2 [Att. 2] [German]).
3.4 Comparison of patients’ and therapists’ perspectives through explorative classification in previously reported theory
In order to be able to compare the results of the patients’ and therapists’ data of the study, the model of embodied aesthetics according to Koch [13] and the therapeutic factor study by De Witte et al. [1] were used: The 103 BTs (considering the frequency of their codes) and the therapists’ statements were both exploratively assigned to the domains of these two models.
3.4.1 Comparison through the model of embodied aesthetics
SK and SE assigned the results to the domains of Koch [13], as reflected in Table 3 [Tab. 3].
Table 3: Basic themes (patients’ data) & therapists' responses assigned to the Model of embodied aesthetics [13]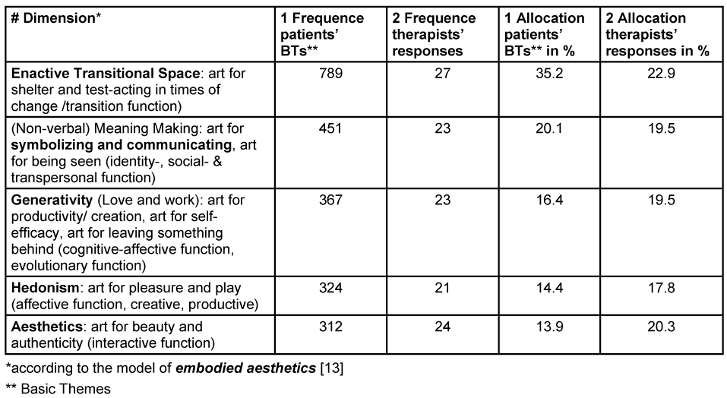
When comparing the Basic Themes (BTs) based on the answers of the patients with the five mechanism clusters in model of embodied aesthetics [13], we found 789 codings of BTs related to enactive transitional space (e.g., safe space, freedom from expectations, being allowed to be, understanding, support, relationship, trust, recognizing patterns, insight into new strategies, rehearsal in movement, embodying emotions, defining boundaries, increasing self-knowledge, change of perspectives, handling problems, transfer to everyday life), 451 codings of BTs related to nonverbal/symbolic communication (e.g., exchange, expression of emotions, access to emotions, lead & follow, proximity & distance), 367 codings of BTs related to generativity (e.g., experiencing self-efficacy, self-competence, self-determination, self-esteem, engagement, freedom), 324 codings of BTs related to hedonism/play (e.g., meeting one’s own needs, letting go mentally and bodily, free movement well-being, exploration) and 312 codings of BTs related to aesthetics (e.g., experiencing wholeness, gratefulness, inner clarity, balance, joy, lightness, strength, energy).
Comparing the answers of the therapists with the five mechanism clusters we found that each cluster was mentioned almost evenly in numbers: the therapists’ statements related 27 times to the enactive transitional space (e.g. discovering new ways of coping, representing boundaries differently), 24 times to aesthetics (e.g., body-mind connection, present attitude/openness, emotion regulation), 23 times to non-verbal/symbolic communication (e.g. social interactions, mirroring) as well as 23 times to generativity (e.g. artistic expression/composing, self-efficacy, activating resources) and 21 times to hedonism/play (e.g. spontaneity, liveliness, emergence).
The clearest difference between patients’ and therapists’ perspectives is that patients emphasized the cluster of enactive transitional space almost twice as much as the other four clusters. The therapists referred to all clusters with almost similar frequency. This suggests that the safe space with possibilities for experimentation, rehearsal in movement, changing perspectives and so on are particularly salient for patients in DMT; thus, this result relates particularly to the process- and experience-orientated approach of DMT which is especially important for the patients when describing its mechanism of change.
3.4.2 Comparison through the 19 identified empirical factor domains of de Witte et al. (2021) [1]
LS and SE exploratively assigned the results to the therapeutic factor domains of De Witte et al. [1]; without any agreement training, the following data resulted (Table 4 [Tab. 4]).
Table 4: BTs (patients' data) & therapists' responses assigned to therapeutic factor domains of De Witte et al. [1]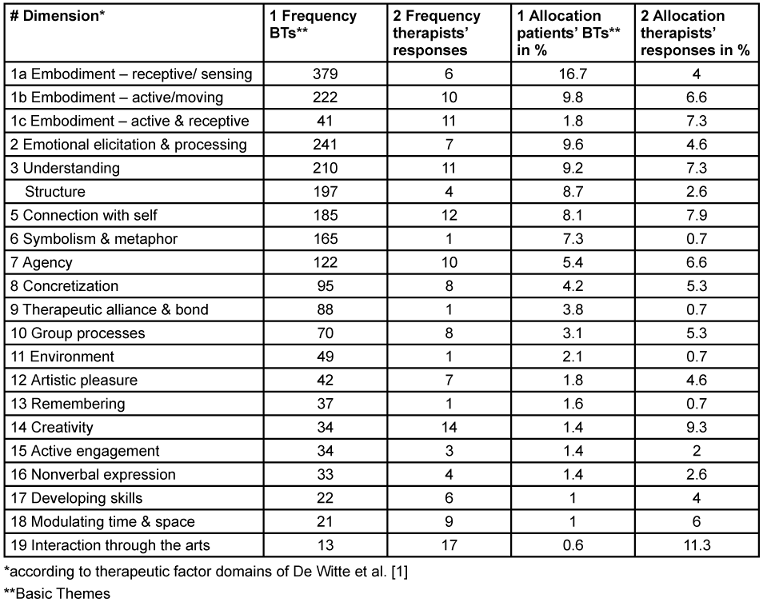
According to the interpretation of the first author the BTs from the patients’ statements (N=748) contained all 19 therapeutic factor domains of De Witte et al. [1] identified in previous empirical studies. The frequency of the BTs in the second column is made up of the number of BTs assigned to the corresponding therapeutic factor domain, taking into account their respective number of codes. For example, three BTs were assigned to the domain Interaction through the arts (n=21): Distraction from problems (n=8), Distraction from pain (n=5), Here & Now (n=8); their frequency of coding was added together. Thereby Embodiment was included in 642 patients’ items as a therapeutic factor and thus was by far the most frequently mentioned one. We divided the category ‘embodiment’ into the active (moving, n=263) and receptive (being moved, n=420) component, to differentiate these two aspects. Notably, 40% of the BTs received multiple assignments, particularly when the two embodiment categories formed one of them.
The therapists’ statements also contained all 19 therapeutic factor domains. According to the frequency of the descriptions of therapeutic factors that can be assigned to the category, embodiment in its receptive component (e.g. body awareness) was mentioned six times, whereas in its expressive component (e.g. active creation) was mentioned ten times. Embodiment as therapeutic factor with its joint (and interactive) receptive and expressive components was named eleven times. Thus, in total, with n=27 mentions, it was the most referenced category by the therapists and often described in combination with other therapeutic factors.
4 Discussion
The present study highlights the central role of dance movement therapy (DMT) as a therapeutic approach that engages a complex interplay of physical, emotional, psychological, cognitive, and social processes [30]. The findings reflect how patients in psychiatric and psychosomatic hospitals in Germany perceive and explain the effects of DMT.
4.1 Therapeutic factors from patients’ perspective in the thematic analysis
The three thematic networks (TNs) identified represent distinct domains of DMT effects experienced by patients:
- Contextual conditions, which patients can influence only to a limited extent (Global Theme [GT] Structure).
- Therapeutic processes relevant for exploring components of the self (GT Self-Exploration).
- Therapeutic factors that allow patients to actively shape their self-concept (GT Self-Management).
4.1.1 The global theme Structure
In addition to the structural framework conditions (OT Design), the GT Structure also encompasses the basic attitude and the way of social interaction of participants involved in the DMT sessions (OTs Atmosphere, Group and Therapist). Patients most frequently emphasized the therapeutic effects of Music (BT), particularly when combined with movement or dance. This finding aligns with Bender’s [33] assertion that music – especially in combination with movement – constitutes a central element of DMT and can be purposefully employed to elicit stimulation or relaxation. Experiencing an accepting atmosphere (BT Being Allowed to Be, n=18) emerged as another key therapeutic factor. According to patients, the therapist plays a pivotal role in creating this environment by providing empathetic guidance, individualized support, psychoeducational input, problem recognition, and task-based impulses. These elements reflect the humanistic principles described by Rogers [34], which underpin many therapeutic processes in DMT.
4.1.2 The global theme Self-Exploration
With 983 codes (compared to Structure: n=364, and Self-Management: n=176), the GT Self-Exploration represented the most significant thematic area for patients. It is based on eight OTs, many emphasizing bodily and movement-related experiences. Notably, the OT Perception accounted for nearly one-quarter of all codes, highlighting the centrality of physical self-awareness in DMT’s therapeutic impact [35]. The most frequently mentioned therapeutic factors were Body awareness (BT), Access to emotions (BT) and Expression of emotions (BT). Adding the aspect of movement (BT) these factors align with the theoretical models of embodied affectivity [3] and embodied aesthetics [13]. These models conceptualize the inseparable connection and reciprocal relationship between perception (reception, impression, affect) and movement (action, expression, emotion), underscoring the inseparability of body and mind [3].
4.1.3 The global theme Self-Management
The GT Self-Management theme captures patients’ descriptions of strengthening their self-concept and related skills. All associated BTs are based on the resource-oriented approach in DMT [36]. However, the distinction between therapeutic factors and outcomes was sometimes ambiguous. For instance, improved self-confidence could be both an outcome of DMT and a therapeutic factor influencing further positive changes, such as enhanced well-being. The most frequently reported BT within this theme was Acceptance. According to Du Bois [37], accepting and acknowledging feelings and body resonances is a principle for strengthening the "Healthy Adult Mode” from schema therapy, which she makes physically tangible for patients in her dance therapy work. Furthermore, patients emphasized a Holistic Approach, connecting body, mind, and spirit, as a core component of the DMT explanatory framework [38]. Patients also described an accepting stance enabling them to integrate the external Being allowed to be (BT from GT Structure, OT Atmosphere) into their own attitude (BT Acceptance).
The comprehensive dataset provides numerous additional insights and interrelations beyond those discussed here. Readers are encouraged to examine the thematic networks for a more detailed understanding.
Perception of inner states, sensing and body awareness promote the detection of inner needs and conditions, authenticity and beauty [18]. Active art-making and creating is a major component influencing the strength of the DMT effects, strengthening the patient’s self-efficacy and agency: From the patient’s perspective, DMT promotes personal responsibility and the activation of resources and skills, and thus contributes to self-efficacy experiences. Those, in turn, are known to have sustainable health benefits [39]. This and other likely therapeutic factor pathways, stated by patients and therapists, can now be tested in subsequent studies.
In the open feedback section of the patient questionnaires, three recurring themes emerged:
- Appreciation of the therapist,
- appreciation of DMT services, and
- practical recommendations for greater accessibility to DMT during and beyond inpatient treatment. Patients consistently expressed the wish that DMT should be made available to all patients.
4.2 Discussion of exploratory results
Embodiment emerged as the most frequently referenced therapeutic factor reported by both patients and therapists, accounting for 28.3% of all coded data when mapped onto the domains of De Witte et al. [1]. While embodiment was consistently emphasized, patients primarily described its receptive component (sensory awareness and interoception), whereas therapists highlighted its active or expressive aspects (movement-based enactment). Is embodiment a higher-order process encompassing other factors, rather than a factor of equal rank? Prior work by Estel and Koch [25] found embodiment to function as a general factor underlying the DMT-SF scale measuring specific therapeutic factors of DMT, suggesting a potentially superordinate role. Further research is needed to define the concept and components of embodiment more clearly, particularly in therapeutic contexts, and to investigate the role of embodiment in relation to other therapeutic factors of DMT in a more differentiated way.
Comparing the most frequently mentioned allocations regarding the 19 domains of De Witte and et al. [1] revealed that patients placed particular emphasis on Emotional elicitation and processing, Understanding, Structure, Connection with self and Symbolism and metaphor, alongside embodiment. Therapists, by contrast, emphasized Interaction through arts, Creativity, Understanding, Connection with the self and Agency. Both groups ranked Understanding/insight and Connection with self among the top six domains. According to De Witte et al. [1], the therapeutic factor domain Connection with self includes aspects like ‘Connection with self through the arts’ and ‘Personal values’, while Understanding encompasses processes such as ‘Self-awareness (through works of art)’ or ‘Meaning Making’ [1]. The overlap in the patients’ and therapists’ data reflect two general therapeutic factors of psychotherapy: finding access to yourself, becoming aware of your patterns (motivational clearance) and identifying one’s resources to support therapeutic change (activation of resources) [40]. Both represent essential mechanisms of change across psychotherapy modalities, including DMT.
Differences in emphasis between patients and therapists likely reflect their distinct roles and perspectives. Patients engage in DMT from a first-person experiential standpoint, focusing on immediate structure, guidance, and newness of the exercises. Therapists, observing from a second-person perspective, are more attuned to interpersonal dynamics, creativity, and agency, which may occur implicitly for patients. Therapists’ theoretical knowledge of DMT allows them to perceive processes not readily verbalized by patients.
Overall, the explorative comparison with previous empirical findings on therapeutic factors of the CATs [1] and the theoretical model of embodied aesthetics [13] suggest that patients’ and therapists’ perspectives jointly cover the full spectrum of these therapeutic factor domains and clusters.
4.3 Methodological discussion and considerations for further research
Our findings prompted several methodological reflections relevant for advancing therapeutic factor research in DMT and the broader CATs field.
4.3.1 Establishing shared terminology
Therapeutic factor research in DMT is still developing, lacking consistent terminology across patients, therapists, and researchers. In this study, we preserved participants’ original phrasing to honor their lived experiences. Future studies should employ participatory approaches to co-construct shared definitions, integrating clinical language with patient experience to improve conceptual clarity and cross-stakeholder communication.
4.3.2 Accounting for the complexity of the change processes when defining specific components
Summarizing the effectiveness of therapeutic treatments in a few sentences is a helpful first step in identifying potential therapeutic factors. However, therapeutic change processes in DMT are multi-layered and often involve interactions between several factors. Patients and therapists frequently described a combination of different therapeutic factors, which could neither be considered independently of each other nor isolated in single categories. To better understand mechanisms of change, future research should employ designs that capture the temporal and relational interplay among factors, such as process-oriented case studies, phenomenological interviews, or longitudinal mixed-methods approaches.
4.3.3 Expanding participatory research approaches to increase learning from patients and therapists
This study amplified the voices of experts by experience by focusing on patient and therapist perspectives. Future research could deepen participation by involving patients in more stages of the research process [41]. Such approaches would democratize therapeutic factor research, foster patient agency, and advance practice-relevant knowledge.
4.3.4 Enhancing practical applicability of therapeutic factors research
The retrospective nature of this study prevented linking specific interventions to specific therapeutic factors. To strengthen theory–practice connections, future research should systematically investigate which interventions activate which factors and how these factors interact (e.g., as mediators or moderators of therapeutic outcomes). Achieving this will require precise, consensus-based definitions and operationalizations of therapeutic factors, enabling the development of testable hypotheses and controlled experimental designs. In this sense, we encourage the scientific community of the CATs to proceed carefully and in agreement when defining and differentiating the concepts used.
4.4. Limitations
Several limitations should be considered. First, voluntary participation may have led to motivational bias, overrepresenting patients with positive attitudes toward DMT. Experiences of disengaged or resistant patients were likely underrepresented. Second, data collection was contingent on therapist availability, resulting in disproportionate abundant contributions from the two therapists included as co-authors. A third limitation is that the patients’ and therapists’ statements were obtained through the open question format in which various experiences over several DMT sessions were summarized. These had different objectives and approaches depending on therapeutic goals or processes of the groups. Patients frequently used non-technical language, making interpretation and categorization of their texts challenging.
The missing control group impeded the comparison with a group that had not received DMT. Future research should try to integrate control groups – a group that receives a form of verbal psychotherapy vs. a group that receives DMT in addition to TAU (treatment as usual just without DMT), for example.
Furthermore, it must be considered that the comparison of patient and therapist rankings of clusters [13] and domains [1] involves different aggregation levels of data, so that its informative value is limited and must be considered exploratory. Considering that the classification was informed by a preliminary and subjective perspective intensive method training is necessary to ensure high interrater reliability.
In addition to the other terms, the factor of embodiment – particularly central according to the results of the study – is often insufficiently defined and too broad a category that actually consists of multiple concepts. In this study, we distinguished active and receptive (motor and sensory) components of it, which leads to more useful data. Another suggestion, resulting from the input of Millman et al. [42], is to differentiate the component of embodiment into interoception and embodied cognition. However here the component of affect linked to embodiment falls short and may require a third differentiation. This is food for thought for future studies.
5 Conclusions
This study examined patient and therapist perspectives on therapeutic factors of DMT in naturalistic clinical settings, including 203 patients across multiple institutions and diagnostic categories (pri-marily depression, pain and anxiety). In sum, based on qualitative patients’ and therapists’ data, findings underscore that embodiment is a key therapeutic factor in the perceived effectiveness of DMT. It was useful to subdivide embodiment into its active and receptive aspects [3], [13].
Results revealed a broad spectrum of therapeutic factors, encompassing general psychotherapeutic mechanisms and DMT-specific processes. These clustered into three categories/general themes:
- the structural frame of the setting providing the general holding environment and specific conditions, including guidance and psychoeducation by the therapists, working with space, using the group as a learning field etc. (Figure 2 [Fig. 2]),
- the self-exploration of the patients, including processes of reflection, perception, opening up and letting go etc. – with the most frequently coded sub-categories of
- the self-management of the patients, comprised of therapeutic factors strengthening the inner self-concept, including aspects of stabilization, self-care and inner attitude (Figure 4 [Fig. 4]).
Patients evaluated the DMT-specific approach through perceptual processes. Those include pro-cesses of Body awareness, which emerged as the most often enumerated therapeutic factor in the TA. Other important factors were the Access to emotions, often achieved through development of the interoception skills and thus through the receptive part of embodiment, and the Expression of emotions as its active part. The predominance of therapeutic factors on the active art-making side show that DMT sustainably builds and supports the agency and self-efficacy beliefs as two of the most important general health predictors, confirmed by the interviews with the dance therapists. The action orientation of DMT, with its proneness to create practice transfer and behavior change, was also emphasized by the therapists.
Patients generally expressed high acceptance of DMT and a desire for expanded outpatient access, particularly for follow-up and aftercare programs. Co-developing such services with patients would align with participatory health research principles [41] and enhance patient-centered care.
In sum, this study contributes empirical evidence supporting embodiment as a central therapeutic factor in DMT and provides exploratory hypotheses for future mechanism research. These findings lay a groundwork for refining theoretical models of DMT, clarifying therapeutic factors, and developing targeted, evidence-informed interventions grounded in patient experience. Patients appreciated DMT, because it addressed them on a holistic body- and strength-based as well as a creative and expressive level. As one therapist aptly observed: "If we start on the body level, we open up a more colorful bouquet of possible resonances to work with.”
Notes
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
The authors would like to express their heartfelt gratitude to all the participants who contributed to the research, as well as to the dedicated therapists who took on the extra effort to integrate the study into their clinical practice. The realization of the study would not have been possible without you. Thank you also to the clinical institutions and the Software AG Stiftung (SAGST, Darmstadt) for supporting the study and thereby making way for clinical research in the field of creative arts therapies.
Contributions
The first author (LS) wrote the first draft focusing on the evaluation of the patients’ responses. The second author (SE) initiated and designed the initial study, conducted and analyzed the therapist interviews and edited the draft. CC was responsible with SK for study coordination, editing the draft and carrying out secondary analyses. SK was involved in designing the initial study with SE and LS, doing secondary analysis and editing the draft. AF and AdB, two DMT therapists, who were not involved in the data analysis part of the study, made significant contributions by collecting data over the course of the study and co-drafting the manuscript.
Informed consent/ethics
The ethical guidelines of the German Psychological Association (DGPs) and the Professional Association of German Psychologists (BDP) were adhered to when conducting the study. Participation in the study was not remunerated and voluntary. The data collected was pseudonymized using a code generated by the patients themselves. Prior to data collection, an application was submitted to the Ethics Committee of the Department of Psychology at the Philipps University of Marburg and received a positive vote (file number: 2021-06k; 22).
Declaration
We used AI for translations (DeepL, Version 1.51.0) and language smoothing of parts of the discussion (Chat GPT-5). All AI-related suggestions were carefully checked and adapted.
References
[1] de Witte M, Orkibi H, Zarate R, Karkou V, Sajnani N, Malhotra B, Ho RTH, Kaimal G, Baker FA, Koch SC. From Therapeutic Factors to Mechanisms of Change in the Creative Arts Therapies: A Scoping Review. Front Psychol. 2021;12:678397. DOI: 10.3389/fpsyg.2021.678397[2] Koch S, Fuchs T, Summa M, Müller C. Body Memory, Metaphor and Movement. Philadelphia: John Benjamins; 2012. DOI: 10.1075/aicr.84
[3] Fuchs T, Koch SC. Embodied affectivity: on moving and being moved. Front Psychol. 2014;5:508. DOI: 10.3389/fpsyg.2014.00508
[4] Bradt J, Shim M, Goodill SW. Dance/movement therapy for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev. 2015 Jan;1(1):CD007103. DOI: 10.1002/14651858.CD007103.pub3
[5] Bräuninger I. Dance movement therapy group intervention in stress treatment: A randomized controlled trial (RCT). Arts Psychother. 2012 Sept;39(5):443-450. DOI: 10.1016/j.aip.2012.07.002
[6] Ho RTH, Fong TCT, Yip PSF. Perceived stress moderates the effects of a randomized trial of dance movement therapy on diurnal cortisol slopes in breast cancer patients. Psychoneuroendocrinology. 2018 Jan;87:119-126. DOI: 10.1016/j.psyneuen.2017.10.012
[7] Koch SC, Mergheim K, Raeke J, Machado CB, Riegner E, Nolden J, Diermayr G, von Moreau D, Hillecke TK. The Embodied Self in Parkinson's Disease: Feasibility of a Single Tango Intervention for Assessing Changes in Psychological Health Outcomes and Aesthetic Experience. Front Neurosci. 2016;10:287. DOI: 10.3389/fnins.2016.00287
[8] Pylvänäinen PM, Muotka JS, Lappalainen R. A dance movement therapy group for depressed adult patients in a psychiatric outpatient clinic: effects of the treatment. Front Psychol. 2015;6:980. DOI: 10.3389/fpsyg.2015.00980
[9] Ho RT, Fong TC, Cheung IK, Yip PS, Luk MY. Effects of a Short-Term Dance Movement Therapy Program on Symptoms and Stress in Patients With Breast Cancer Undergoing Radiotherapy: A Randomized, Controlled, Single-Blind Trial. J Pain Symptom Manage. 2016 May;51(5):824-31. DOI: 10.1016/j.jpainsymman.2015.12.332
[10] Karkou V, Aithal S, Richards M, Hiley E, Meekums B. Dance movement therapy for dementia. Cochrane Database Syst Rev. 2023 Aug;8(8):CD011022. DOI: 10.1002/14651858.CD011022.pub3
[11] Bräuninger I. The efficacy of dance movement therapy group on improvement of quality of life: A randomized controlled trial. Arts Psychother. 2012 Sept;39:296-303. DOI: 10.1016/j.aip. 2012.03.008
[12] Koch SC, Riege RFF, Tisborn K, Biondo J, Martin L, Beelmann A. Effects of Dance Movement Therapy and Dance on Health-Related Psychological Outcomes. A Meta-Analysis Update. Front Psychol. 2019;10:1806. DOI: 10.3389/fpsyg.2019.01806
[13] Koch SC. Arts and health: Active factors and a theory framework of embodied aesthetics. The Arts in Psychotherapy. 2017;54: 85-91. DOI: 10.1016/j.aip.2017.02.002
[14] Koch SC. Embodiment: Der Einfluss von Eigenbewegung auf Affekt, Einstellung und Kognition. Experimentelle Grundlagen und klinische Anwendungen. Berlin: Logos; 2011.
[15] Fuchs T. Leib, Raum, Person: Entwurf einer phänomenologischen Anthropologie. Stuttgart: Klett-Cotta; 2000.
[16] Merleau-Ponty M. Phänomenologie der Wahrnehmung. Leipzig: De Gruyter; 1962.
[17] Neumann R, Strack F. Approach and avoidance: the influence of proprioceptive and exteroceptive cues on encoding of affective information. J Pers Soc Psychol. 2000 Jul;79(1):39-48. DOI: 10.1037//0022-3514.79.1.39
[18] Caldwell C. Bodyfulness: Somatic Practices for Presence, Empowerment, and Waking up in This Life. Boulder, CO: Shambhala Publications; 2018.
[19] Caldwell C, Leighton LB. Oppression and the Body: Roots, Resistance, and Resolutions. Berkeley, CA: North Atlantic Books; 2018.
[20] Payne H, Koch SC, Tantia J, Fuchs T. The Routledge International Handbook of Embodied Perspectives in Psychotherapy: Approaches from Dance Movement and Body Psychotherapies. London: Routledge; 2019. DOI: 10.4324/9781315159416
[21] Koch SC, Fischman D. Embodied Enactive Dance/Movement Therapy. American Journal Of Dance Therapy. 2011 Apr 26;33(1):57-72. DOI: 10.1007/s10465-011-9108-4
[22] Liang CX, Bryant T. The Use of Dance and Movement for the Embodied Healing of Interpersonal Trauma in Women and Girls: A Systematic Review. Trauma Violence Abuse. 2024 Oct;25(4):3241-3253. DOI: 10.1177/15248380241243399
[23] Koch S. “Being Moved” as a Therapeutic Factor of Dance Movement Therapy. In: Wengrower H, Chaiklin S, editors. International perspectives on dance and creative process in DMT. New York: Routledge; 2021. p. 96-110. DOI: 10.4324/9780429442308-10
[24] Wilson M. Six views of embodied cognition. Psychon Bull Rev. 2002 Dec;9(4):625-36. DOI: 10.3758/bf03196322
[25] Estel SM, Koch SC. Wirkfaktoren von Tanz- und Bewegungstherapie im klinischen Kontext [Therapeutic Factors of Dance Movement Therapy in clinical context]. Die Psychotherapie. 2023; 68: 280-288. DOI: 10.1007/s00278-023-00661-x
[26] Vogel E, Blanck P, Bents H, Mander J. Wirkfaktoren in der Gruppentherapie: Entwicklung und Validierung eines Fragebogens [Change Factors in Group Therapy: Development and Validation of a Questionnaire]. Psychother Psychosom Med Psychol. 2016 May;66(5):170-9. DOI: 10.1055/s-0042-104495
[27] Attride-Stirling J. Thematic networks: an analytic tool for qualitative research. Qual Res. 2001 Dec;1(3):385-405. DOI: 10.1177/146879410100100307
[28] Braun V, Clarke V. Thematic analysis. In: Cooper H, Camic PM, Long DL, Panter AT, Rindskopf D, Sher KJ, Herausgeber, editors. APA handbook of research methods in psychology, Vol 2: Research designs: Quantitative, qualitative, neuropsychological, and biological. Washington: American Psychological Association; 2012. p. 57-71.
[29] Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006;3(2):77-101. DOI: 10.1191/1478088706qp063oa
[30] Berufsverband der TanztherapeutInnen Deutschlands e.V. (BTD). Der tanztherapeutische Prozess. [accessed 2025 Jan 01]. Available from: http://www.btd-tanztherapie.de/index.php?cid=366&pid=347
[31] Estel SM. Erhebung der Wirkweise von Tanz- und Bewegungstherapie im klinischen Kontext - eine Befragung von Patient*innen nach dem Mixed-Methods Ansatz [Masterarbeit]. Marburg: Universität Marburg; 2022.
[32] Roth G. Sweat Your Prayers: Movement as Spiritual Practice. New York: Jeremy P. Tarcher/Putnam; 1998.
[33] Bender S. Grundlagen der Tanztherapie. Gießen: Psychosozial-Verlag; 2020. DOI: 10.30820/9783837927658
[34] Rogers CR. Die klientenzentrierte Gesprächsttherapie. Client-Centered Therapy. Frankfurt am Main: Fischer; 1983.
[35] Geuter U. Praxis Körperpsychotherapie: 10 Prinzipien der Arbeit im therapeutischen Prozess. Berlin: Springer-Verlag; 2018. DOI: 10.1007/978-3-662-56596-4
[36] Eberhard-Kaechele M. Ressourcenorientierung in der Tanz-und Ausdruckstherapie. In: Perlen des Lebens und Selbst-Wert-Schöpfung: Beiträge der 11. und 12. Fachtagung der Gesellschaft für Biodynamische Psychologie/Körperpsychotherapie. Gesellschaft für Biodynamische Psychologie/Körperpsychotherapie (GBP e.V.), editor. Norderstedt: Books on demand; 2010. p. 83-107.
[37] Du Bois A. Fachbeitrag: Schematherapeutische Aspekte in der Tanztherapie. Körp - Tanz - Beweg. 23. 2022 Jun;10(3):101-13. DOI: 10.2378/ktb2022.art15d
[38] Fogel A. Selbstwahrnehmung und Embodiment in der Körperpsychotherapie. Stuttgart: Schattauer; 2018.
[39] Schwarzer R, Jerusalem M. Das Konzept der Selbstwirksamkeit. In: Selbstwirksamkeit und Motivationsprozesse in Bildungsinstitutionen. Weinheim: Beltz; 2002. p.28-53.
[40] Grawe K, Donati R, Bernauer F. Psychotherapie im Wandel: von der Konfession zur Profession. 5., unveränd. Aufl. Göttingen: Hogrefe; 2001.
[41] Wright MT. Was ist Partizipative Gesundheitsforschung? Prävention und Gesundheitsförderung. 2013;8(3):122–31. DOI: 10.1007/s11553-013-0395-0
[42] Millman LSM, Hunter ECM, Orgs G, David AS, Terhune DB. Symptom variability in depersonalization-derealization disorder: A latent profile analysis. J Clin Psychol. 2022 Apr;78(4):637-655. DOI: 10.1002/jclp.23241
Attachments
Erratum
- Minor edits to the wording were made in sections 2.2.1 and 2.2.2.
- Additions and updates to “Acknowledgements” and “Contributions” under Notes.

