The WMA Declaration of Helsinki – Revision 2024: A synopsis and perspectives for professionals in the domain of medical informatics, biometry, and epidemiology
Nils Freyer 1Myriam Lipprandt 1
Andreas Goldschmidt 2
Dominik Groß 3
Rainer Röhrig 1
1 Institute of Medical Informatics, Medical Faculty, RWTH Aachen University, Aachen, Germany
2 Institute for Occupational, Social and Environmental Medicine, Goethe University Frankfurt, Frankfurt, Germany
3 Institute for the History, Theory and Ethics of Medicine, Medical Faculty, RWTH Aachen University, Aachen, Germany
Abstract
Background: Sixty years after its introduction in 1964, the Declaration of Helsinki (DoH) was once more revised in 2024. In this article, we provide a brief historical overview followed by an introduction to the DoH to the interdisciplinary and interprofessional domains of medical informatics, biometry, and epidemiology.
Methods: We performed a critical synopsis of the 2013 and 2024 versions of the DoH, discussing the adequacy of the updates to existing and emerging challenges of medical research in the domain of medical informatics, biometry, and epidemiology.
Results: Major updates of the new version are the extension of the scope of addressees to all researchers related to medical research involving human participants. Further, it adapts terminological changes from the current discourse in applied ethics and strengthens demands for sustainability and equity. The responsibility of researchers is extended to encompass society as a whole, beyond the study population. It does not explicitly include principles on artificial intelligence (AI) in medical research. However, its principles are applicable to AI and address many AI relevant points.
Discussion: In comparison to the 2013 version, the 2024 version of the DoH shows significant improvements concerning the role of participants, sustainability, and justice. To implement the extended scope of addressees, it poses new challenges to policy making in professional laws or associations and societies to adapt the DoH in their rules of conduct. Concerns on AI in medical research seem to be largely covered by existing articles of the DoH. Still, having explicit ethical guidelines for using AI in medical research could be helpful in working out specific recommendations for dealing with the risks and possibilities of AI.
Keywords
codes of ethics, ethics, Helsinki Declaration, Nuremberg Code, ethics committees
1 Introduction and historical milestones
Today more than ever, interdisciplinarity and internationality are key prerequisites for the exchange of current research findings and technical developments in healthcare. The German Society for Medical Informatics, Biometry and Epidemiology (GMDS), for example, has traditionally been involved in this ongoing transfer of knowledge between its specialist areas for decades, which have been and continue to be supplemented by other disciplines such as medical documentation, bioinformatics, and public health [1]. The diversity of interdisciplinary and interprofessional collaborating disciplines and specializations is a particular challenge when it comes to observing ethical concerns and principles, especially because these are subject to an ongoing discourse and thus, continuously changing.
The Declaration of Helsinki (DoH) comprises a set of ethical principles developed by the World Medical Association (WMA) as guidelines for medical research involving human subjects. It is now widely regarded as the fundamental document on ethics in research involving human subjects [2].
The original version of the DoH was based on the principles of the Nuremberg Code (1947) [3], [4], [5], [6], which was introduced after the Second World War as the first generally recognized and accepted code of ethics for medical research involving human subjects (cf. Appendix B in Attachment 1 [Att. 1]). The Nuremberg Code was the result of the Nuremberg Doctors’ Trial of 1946/1947, in which doctors were accused and, in some cases, convicted of “war crimes” and “crimes against humanity” during the Nazi dictatorship [6], [7]. The ten-point code was part of the judgement and pronouncement handed down on 19 August 1947. In fact, the code was used in Nuremberg to justify the verdicts handed down; however, in view of its fundamental importance for medical research practice, it subsequently gained worldwide attention and recognition as an independent text. The Code’s influence is evident not least in the fact that in 1997, 50 years after the verdict in the Doctors’ Trial was announced, a “Nuremberg Code 1997” was published. It was written by a group of doctors from the IPPNW (International Physicians for the Prevention of Nuclear War). They took the anniversary as an opportunity to recall the fundamental principles of the 1947 code and relate them to contemporary medical ethics issues [8].
The Nuremberg Code ultimately served not only as a reference point for the first version of the DoH (1964), but also for the Bioethics Convention of the Council of Europe (1999), hereinafter referred to as Oviedo Convention, which is also discussed in the context of the DoH [9] (see Figure 1 [Fig. 1] and Table 1 [Tab. 1]). The Oviedo Convention was and is – with regard to the protection of human dignity and human rights in Europe – to be understood merely as a minimum standard [10] (see Table 2 [Tab. 2]). It is not considered sufficient by all member states. Only 34 of the 47 member states of the Council of Europe have signed the convention to date, with 26 additional states having ratified it. Of the German-speaking countries, only Switzerland has signed and ratified the international treaty to date. A key point of criticism can be found in Article 17 (‘Protection of persons unable to give consent in research projects’): this article opens up the possibility of research involving persons who are unable to give consent – a particularly controversial aspect of biomedical research [9].
Figure 1: Venn diagram illustrating the overlaps between the Oviedo Convention, the Nuremberg Code, and the Declaration of Helsinki; schematic, not quantitative (cf. Table 2). The Nuremberg Code ultimately served not only as a reference point for the first version of the DoH (1964), but also for the Oviedo Convention (1999), which is also discussed in the context of the DoH [9]. The 2024 version of the Declaration of Helsinki represents a significant further development of ethical standards for medical research. It expands the scope of responsibility, strengthens the rights and protection of participants, and integrates contemporary ethical considerations on sustainability and scientific integrity. These changes are intended to ensure that medical research is ethical, participant-centered, and beneficial to society while adhering to rigorous scientific standards.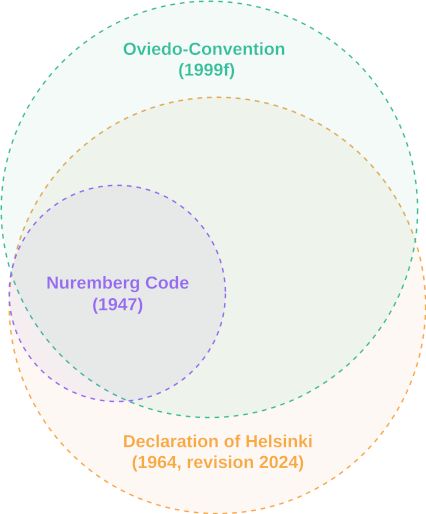
Table 1: As the only international legally binding instrument on the protection of human rights in the biomedical field, the Oviedo Convention [10] establishes fundamental principles to safeguard human dignity in the rapidly evolving domains of biology and medicine. Through these principles, the Oviedo Convention aims to ensure that developments in biomedicine benefit future generations and all of humanity while protecting fundamental human rights and dignity in this rapidly evolving field.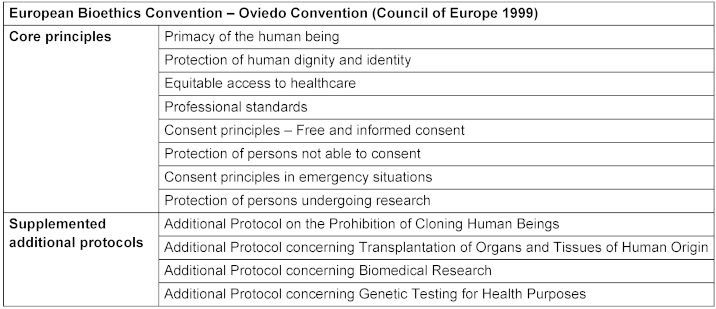
Table 2: Intersections and differences of some principals (see Figure 1: Venn diagram) of Helsinki (DoH 2024), Oviedo (1999) and Nuremberg Code (1947). All three declarations share the principles of voluntary, informed consent, the primacy of the individual, the protection of dignity and rights, the qualification of researchers and the right to withdraw from participation. Nuremberg and Helsinki focus on social benefits. The Oviedo Convention and the Declaration of Helsinki particularly concern dealing with vulnerability, equitable healthcare, and the role of ethics committees.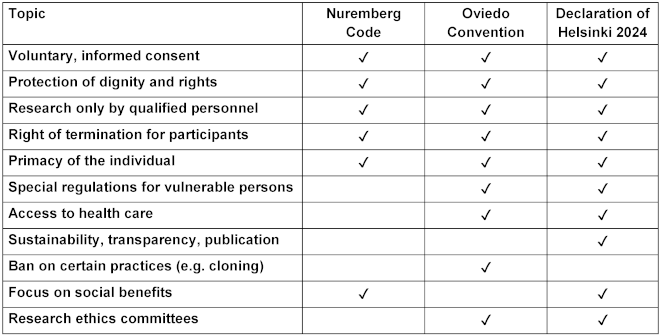
Unlike the Nuremberg Code, which was primarily formulated for the purpose of adjudication, and the said Council of Europe initiative, the DoH was the first explicit initiative by the medical community to standardize ethical research practices. The first version of the declaration was adopted in Helsinki, Finland, in 1964. At the time, however, it met with a mixed response because it still had clearly paternalistic features. Although a distinction was made between therapeutic experiments and clinical research, the right to medical freedom of treatment was reaffirmed: the informed consent of the patient was to be obtained only if it was possible and ‘reasonable’ from a medical point of view [9]. Since then, the DoH has been revised and clarified several times to take account of the changing framework conditions of medical ethics and research practice, but also of cultural and social changes in the relationship between patient and doctor (establishment of patient autonomy as a central ethical principle). While it initially differed from the Nuremberg Code primarily in relation to informed consent, moving from ‘absolutely necessary’ to ‘if possible’ and allowing proxies [11], the declaration has evolved considerably over the last few decades from 11 to 37 articles and has thus undergone a series of changes.
Sixty years after its original introduction, the DoH was revised for the 8th time in 2024. There were 8 revisions and 2 clarifications to date, making the 2024 DoH the 11th version [12]. While organizations active in human-research already adopt the DoH even for non-healthcare professionals – the German Association for Medical Informatics, Biometry and Epidemiology requires all its members to know and act upon the declaration in their ethical guidelines [13] – it is the first time that the WMA explicitly addresses non-healthcare-professional researchers with the DoH. Therefore, in addition to this historical contextualization, this article aims to introduce the DoH and discuss it critically, with a focus on medical informatics, biometry, and epidemiology.
Beyond that, we identify key differences between the DoH revisions of 2013 (Fortaleza) and 2024 (Helsinki). It is of particular interest to identify and discuss the changes in terms of their relevance to medical data science. A systematic synopsis of the 2023 and the 2024 version of the DoH can be found in Appendix A in Attachment 1 [Att. 1].
2 The Declaration of Helsinki in 2013 and 2024: Content and updates
The DoH revision 2024 is subdivided into a preamble and a section of general principles, further differentiated by ten subsections. The WMA states that the declaration should be read as a whole, the complete declaration can be found on the WMA’s website [12]. In the following, there will be a brief introduction to its contents to provide an overview on the topics covered by the DoH and to better embed the updates we will report and discuss thereupon.
2.1 General principles of the DoH
The DoH prioritizes the well-being of individuals over the interests of science and society (Art. 7), advocating for the minimization of risks and burdens and the need to show that the associated risks and burdens are justified by the supposed benefits of the research conducted (Art. 16–18). It emphasizes the necessity of conducting research based on scientifically sound protocols (Art. 22), which must be reviewed and approved by independent research ethics committees (RECs) to safeguard participants’ protection (Art. 23). Article 23 further specifies that the ethics committees must “take into consideration the ethical, legal, and regulatory norms and standards of the country or countries in which the research is to be performed as well as applicable international norms and standards”, however, emphasizing that those may not overrule the protections of the patient set forth in the DoH. An important principle of the DoH is the requirement for informed consent, requiring that participants or their proxies are fully aware of the study’s purpose, procedures, potential risks, benefits, and burdens before agreeing to participate (Art. 25–32). Additionally, it underscores the importance of maintaining participant privacy and confidentiality (Art. 24) and addresses the specific needs and protections required for individuals, groups, and communities in situations of vulnerability, while generally advocating for their inclusion in medical research (Art. 19–20).
Beyond participant protection, the DoH highlights aspects of scientific integrity, global justice, and ecological sustainability. It advocates for the responsibility of “researchers, authors, sponsors, editors, and publishers” to ensure transparency and integrity in their work (Art. 35–36). This includes the obligation to publish all research findings, whether positive or negative, to contribute to the collective scientific knowledge and prevent duplication of efforts (Art. 36). The declaration further acknowledges that medical research is inherently embedded in structures of social inequalities and calls for the equitable distribution of the benefits, risks, and burdens resulting from the conduct and results of medical research (Art. 6). It addresses the need for ongoing ethical oversight, adaptation to new scientific advancements, and the declaration’s applicability across diverse cultural and social contexts.
2.2 Qualitative analysis of the changes
The 2024 version of the DoH clearly updated its terminology. There is a shift in terminology from “subjects” to “participants”, reflecting a more participant-centered approach that emphasizes voluntariness and respect for autonomy. Further, the 2024 version extends the ethical obligations not only to physicians but to all researchers involved in medical research, indicating a broader application of ethical standards. Lastly, the new version places greater emphasis on certain ethical considerations, particularly in relation to autonomy, privacy, and the rights of participants, as well as considerations of justice. This includes a more explicit mention of scientific integrity and the need to avoid misconduct in research. The main changes are summarized in Table 3 [Tab. 3].
Table 3: Main changes found in the qualitative analysis of the synopsis of the 2013 and the 2024 DoH. The complete synopsis can be found in Appendix A in Attachment 1.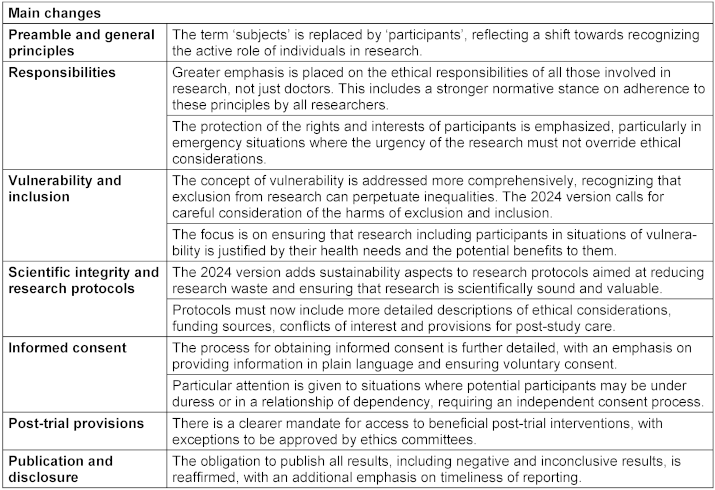
2.3 Interpretation of the updates
In the following, we discuss our interpretation of the changes in the updated DoH compared to 2013, particularly regarding their significance for the fields of medical informatics, biometry, and epidemiology.
2.3.1 The new role of researchers
One of the attention drawing updates of the 2024 DoH is the extension of the scope from physicians to “all individuals, teams, and organizations involved in medical research” (Art. 2) within the declaration’s preamble. The 2013 version was primarily directed at physicians in its preamble and included other healthcare professionals in individual articles (see Arts. 9 and 12). Throughout the new version, articles that do not face aspects of medical research specific to physicians or other healthcare-professionals (e.g. Art. 14) are adapted accordingly [14], [15], [16] (cf. Arts. 2, 6, 9, 10, 12, 18, 20, 22, 31). It therefore adapts to the Council for International Organizations of Medical Sciences’ 2016 International Ethical Guidelines for Health Research Involving Humans [17], [18]. At the same time, however, it clearly goes beyond the original scope, which was characterized by the fact that the World Medical Association formulated regulations for its professional representatives – doctors – but not for members of other professions.
By that, if implemented, the 2024 DoH sets new requirements for researchers from medical informatics, biometry, and epidemiology:
- considering an equal distribution of risks, burdens, and benefits across communities (Art. 6),
- partaking in the active protection of the participants (Arts. 6 and 9),
- considerations of ethical, legal, and regulatory standards (Art. 10),
- supervising ethical research conduct (Art. 12),
- assessing the management and balance of risks, burdens, and benefits (Art. 18),
- assessing the disparities between populations, especially in situations of vulnerability (Art. 20),
- providing transparent information on qualifications in the research protocol (Art. 22),
- and the responsibility to obtain informed consent by potential participants (Art. 31).
The DoH is not a legally binding policy, however, it largely influenced regulations as, among others, the clinical trials regulation of the European Union [19]. It must be seen to what extent the extension of the role responsibility of other researchers translates to policy updates in their respective professional law or codes of conduct. Especially regarding RECs, obligatory supervision for medical research is required by physicians’ professional law. However, as there is no professional law that applies to all non-medical researchers, a generalization of such legal obligation would require an adapted legal framework. Regardless of the respective professional law, compliance with the principles of the DoH morally requires consultation with RECs even for studies without the participation of physicians.
In terms of terminology, the most notable update in the 2024 DoH is the replacement of “human subjects” by “participants”, emphasizing the voluntariness as well as “the rights, agency, and importance of those individuals as partners in the research enterprise” [16].
2.3.2 Strengthening the ethics committees
The 2024 DoH significantly updates Art. 23 on RECs. First, the 2024 version further emphasizes the independence of the RECs by stressing sufficient resources and adequate qualifications. Second, the focus of the ethics committees has been expanded from “laws and regulations” to “ethical, legal, and regulatory norms”. Third, the 2024 version now explicitly requires the RECs of all countries involved in international research to approve the research project. Finally, the required rights of RECs have been extended to withdraw approval from ongoing research and to suspend ongoing research:
In consequence, the right to monitor ongoing research more strictly may allow for a change in the policy for continuous research. One example is the Data Use and Access Committee (DUAC), which reviews applications for the use of registry data. Currently, each individual use of data must also be approved by the REC. However, if the RECs were more closely involved in the work of the DUAC, it could delegate certain tasks to this body. The prerequisite for this is that the DUAC complies with defined quality standards. In this case, many applications could be processed without further review by the REC. This delegation could ease the workload on ethics committees and researchers while ensuring that reporting obligations and monitoring mechanisms are maintained. Monitoring and control mechanisms can be implemented on an as-needed basis or spontaneously, allowing for a flexible response to emerging situations and random sample interventions. This framework provides the opportunity for intervention or withdrawal of approval if necessary.
2.3.3 Extending the scope beyond individuals
A frequently discussed update of the DoH that runs through many parts of the declaration is the update of the scope beyond individuals [20], [21].
The 2024 version supplements the minimization of environmental damage with the pursuit of ecological sustainability and emphasizes that this must already be considered in the design (Art. 11). An important addition, as minimizing damage to the environment is insufficient to achieve ecological sustainability. Further, in Art. 21, the updated version adds that justified medical research must be promising and waste reducing.
Moreover, the updated DoH strengthens its emphasis on structural injustices. Art. 6, stresses the context of inequities that medical research takes place in and adds that the distribution of the benefits, risks, and burdens requires ethical examination. It also introduces communities as important stakeholders in medical research and states that participants and their communities must be involved in research design and implementation (Art. 6). These changes address structural injustices caused by power relations between researchers and participants as well as structural inequalities. The updated version no longer advocates only for the protection of such groups, individuals, or communities, but also explicitly for their inclusion in research projects. The potential harm caused by exclusion must now be weighed against the potential harm caused by inclusion (Art. 19), and inclusion should be sought in particular if exclusion would lead to increased inequality (Art. 20).
Another noteworthy change is the DoH’s significantly updated section on vulnerability. Besides a more sensible use of the terminology of vulnerability, seemingly aiming to avoid stereotyping and over-generalization, the updated version acknowledges that the rigorous exclusion due to situations of vulnerability poses the strong risk of under-representation and missing knowledge on special health needs (Art. 19 and 20).
Finally, the conditions of informed consent are adapted to highlight inclusivity: potential participants must be informed in simple language about the objectives, methods, expected benefits and possible risks and burdens (Art. 26). The inclusion of participants in situations of vulnerability was adapted to now allow for inclusion even if incapable of giving informed consent, given that “the research is likely to either personally benefit them or if it entails only minimal risk and minimal burden” (Art. 28).
2.3.4 Artificial intelligence and the Declaration of Helsinki
In its updated version from 2024, the DoH does not explicitly address ethical concerns relating to artificial intelligence (AI) in healthcare or health research.
With regard to the use of artificial intelligence in healthcare, ethicists have extensively examined the implications of this disruptive technology and discussed, for example, explicability or explainability as a genuine ethical principle [22], [23], [24]. In addition, the literature on the ethics of AI in healthcare deals with concerns such as biases, non-reproducible or non-generalizable results [25], and problems in the assignment of responsibility [26]. In a recent position paper on AI in healthcare, for example, the German Medical Association asserts that the development of AI in healthcare is driving the digitization of healthcare and producing huge amounts of training data that sometimes conflict with privacy and data protection [27]. On the one hand, some argue that a correct and differentiated implementation of the principles set out in the DoH takes into account the risks of AI analysis and development [21], [28], [29]. On the other hand, others claim that the updated DoH does not address the need for specific issues related to “artificial intelligence or machine learning research” [14]. Ribeiro specifically criticizes that the updated DoH is missing guidance on AI related concerns on “data privacy, algorithmic bias, and the role of machine learning in clinical decision making” [30].
Article 6 of the DoH 2024 calls for a fair distribution of risks, burdens, and benefits, which in principle also includes the avoidance of biases. The update to the DoH also covers the relevance of including groups and individuals in situations of vulnerability to avoid disadvantages (Art. 19, 20). However, the declaration does not specify any technical causes or corrective mechanisms for such distortions, which can arise in AI systems due to non-representative training data or model architectures. Additional guidelines are therefore required for practical implementation, for example on data representativeness.
Concerns about the explainability of AI models in medicine relate primarily to their use in diagnostics and therapeutic decision-making [24]. This also affects research that investigates the practical application of AI. The DoH requires that participants be sufficiently informed to voluntarily consent to a study (Art. 25–32). Non-explainable AI could make such consent difficult. On the other hand, the declaration does not specify what “sufficiently informed” means in the context of complex AI models. In practice, such models are often accepted. However, there is still no consensus in the ethical discussion on the necessity and degree of explainability [24].
Article 9 of the DoH declares that responsibility for the protection of participants always lies with the researchers. It thus defines a procedure for assigning responsibility that is not trivial in the case of AI and requires researchers to actively take responsibility as a basic prerequisite for the use of AI in research. To legitimize such assignment of (moral) responsibility, control mechanisms are needed that limit the autonomy of decision-making by AI (e.g., Human in the Loop [31]).
The use of large amounts of data and their secondary exploitation are also a central topic of AI research. While the DoH remains rather general in this regard, the Declaration of Taipei [32] offers a much more differentiated ethical basis for the handling of health data. It is therefore an important addition for data-intensive AI projects, which is referenced in Art. 32 of the DoH.
Thus, the use of artificial intelligence (AI) in medical research is only ethically justifiable if central principles such as patient autonomy, justice, fairness, and epistemological standards are upheld. These requirements can generally be reconciled with the normative guidelines of the DoH. To our knowledge, there are no ethical concerns in the context of AI in medical research that are not at least implicitly addressed by the existing principles of the declaration. In particular, the technology-independent wording of the declaration allows for a broad interpretation that also encompasses novel research approaches such as the use of AI. Nevertheless, it can be argued that disruptive technologies such as AI in particular require additional ethical guidelines to address specific challenges, such as lack of explainability, distributed responsibility, or data ethics issues.
3 Discussion
While many local guidelines for non-medical human researchers already reference the DoH, the updated version now explicitly addresses them. In that light, the role of researchers is further differentiated in the 2024 version. At the same time, the target group of DoH is significantly expanded through the explicit inclusion of all researchers. The extension of the scope of the DoH does not naturally translate into binding policy but may pave the way to a legal framework that is not restricted to professional law but sets the legal basis for research on human participants. For instance, supervision by RECs may be obligatory to any researcher involved in human research. An example for such a legal basis can be found in the Human Research Act of Switzerland [33].
The DoH in its current version also extended the scope beyond individuals, i.e., patients, and explicitly calls for ethical principles to address inequities and climate change. Further, it is noticeable that the adoption of conceptual discourses has found its way into the updates (e.g. for ‘vulnerability’ and ‘autonomy’ see Appendix A in Attachment 1 [Att. 1], Arts. 9, 19, 20).
The ethical challenges arising from the use of AI in medical research can largely be addressed by the principles of the DOH, provided that these are interpreted independently of technology. Nevertheless, given the specific characteristics of disruptive technologies such as AI, consideration should be given to developing supplementary ethical guidelines that clarify existing standards and specify their application in practice.
In the context of medical data, however, we may still criticize a lack of guidance for studies in clustered settings: An increasing number of studies are being conducted under conditions that can only be implemented in a clustered manner, rendering individual patient consent challenging [34]. Furthermore, information technology intervenes embedded healthcare processes, making it sometimes impossible to exclude individual patients. As a result, informed consent is compromised, highlighting a pressing need for policy development. While this is not necessarily the task of the DoH, especially as the WMA does not represent the domains of medical informatics, biometry, and epidemiology, questions remain unanswered, stressing the need for further discussions.
Notwithstanding the current update, the standardization of research involving humans must be viewed as a time- and context-dependent process that requires constant evaluation and further development, as well as ongoing discursive debate. The real challenge lies in applying existing standards to specific cases [9].
Lastly, this article only focuses on selected updates and key points of the DoH, relevant to the domains of medical informatics, biometry, and epidemiology, only providing partial insights.
Notes
Acknowledgements
We would like to thank the WMA for the copyright permission to publish the complete synopsis.
Authors’ ORCIDs
- Nils Freyer: 0000-0002-4460-3650
- Myriam Lipprandt: 0000-0001-9371-0551
- Andreas Goldschmidt: 0009-0004-5073-6806
- Dominik Groß: 0000-0001-9979-8531
- Rainer Röhrig: 0000-0002-0032-5118
Author contributions
NF, RR idea, design, conception of the work. NF, RR performed the formal analysis. All authors interpreted the results. NF wrote the manuscript (draft). All authors reviewed and edited the manuscript.
Competing interests
The authors declare that they have no competing interests.
References
[1] Goldschmidt A, Deserno TM, Winter A, Gerecke BJ. 22 Elemente eines Ethikkodex für Medizin- und Informationstechnische Fachgesellschaften. In: Ethische Perspektiven auf Biomedizinische Technologie. De Gruyter; 2020. p. 233-245. DOI: 10.1515/9783110645767-022[2] Bošnjak S. The declaration of Helsinki: The cornerstone of research ethics. Arch Oncol. 2001;9(3):179-184.
[3] The Nuremberg Code (1947). BMJ. 1996 Dec 7;313(7070):1448. DOI: 10.1136/bmj.313.7070.1448
[4] Annas GJ, Grodin MA, editors. The Nazi Doctors and the Nuremberg Code: Human Rights in Human Experimentation. Oxford University Press; 1992. DOI: 10.1093/oso/9780195070422.001.0001
[5] Weindling P. The origins of informed consent: the International Scientific Commission on Medical War Crimes, and the Nuremburg code. Bull Hist Med. 2001;75(1):37-71. DOI: 10.1353/bhm.2001.0049
[6] Groß D. Nürnberger Kodex. In: Lenk C, Duttge G, Fangerau H, editors. Handbuch Ethik und Recht der Forschung am Menschen. Berlin, Heidelberg: Springer; 2014. p. 559-563. DOI: 10.1007/978-3-642-35099-3_88
[7] Roelcke V, Maio G, editors. Twentieth century ethics of human subjects research: historical perspectives on values, practices, and regulations. Franz Steiner Verlag; 2004.
[8] Deutsche Sektion der Internationalen Ärzt*innen für die Verhütung des Atomkrieges/Ärzt*innen in sozialer Verantwortung e.V. (IPPNW). Nürnberger Kodex (1997). Dokumente und Erklärungen. [cited 2025 Apr 22]. Available from: https://www.ippnw.de/der-verein/geschichte-der-ippnw/erklaerungen/artikel/de/nuernberger-kodex-1997.html
[9] Groß D. Forschung am Menschen. In: Neuhäuser C, Raters ML, Stoecker R, editors. Handbuch Angewandte Ethik. Stuttgart: J.B. Metzler; 2023. p. 719-726. DOI: 10.1007/978-3-476-05869-0_97
[10] Council of Europe. Convention for the protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine (ETS No. 164). Treaty Office; 1999 [cited 2025 Apr 22]. Available from: https://www.coe.int/en/web/conventions/full-list
[11] WMA – The World Medical Association. Declaration of Helsinki 1964. 1964 [cited 2025 Feb 13]. Available from: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/doh-jun1964/
[12] WMA – The World Medical Association. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Participants. 2024 [cited 2024 Dec 17]. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki/
[13] Deutsche Gesellschaft für Medizinische Informatik, Biometrie und Epidemiologie (GMDS). Ethische Leitlinien. GMDS; 2008.
[14] Bierer BE. Declaration of Helsinki-Revisions for the 21st Century. JAMA. 2025 Jan;333(1):18-19. DOI: 10.1001/jama.2024.22281
[15] Zhang H, Wu Y, Wang H, Zhao W, Cong Y. Sixty years of ethical evolution: The 2024 revision of the Declaration of Helsinki (DoH). Health Care Sci. 2024 Dec;3(6):371-373. DOI: 10.1002/hcs2.126
[16] Resneck JS Jr. Revisions to the Declaration of Helsinki on Its 60th Anniversary: A Modernized Set of Ethical Principles to Promote and Ensure Respect for Participants in a Rapidly Innovating Medical Research Ecosystem. JAMA. 2025 Jan;333(1):15-17. DOI: 10.1001/jama.2024.21902
[17] Rägo L, Sawyer J. Keeping ethical pace with medical research: the 10th revision of the Declaration of Helsinki. BMJ. 2025 Jan;388:r9. DOI: 10.1136/bmj.r9
[18] The Council for International Organizations of Medical Sciences (CIOMS). 2016 International ethical guidelines for health-related research involving humans. Geneva: CIOMS; 2016. DOI: 10.56759/rgxl7405
[19] Regulation (EU) No 536/2014 of the European Parliament and of the Council of 16 April 2014 on clinical trials on medicinal products for human use, and repealing Directive 2001/20/EC. Text with EEA relevance. OJ L Apr 16, 2014. Available from: http://data.europa.eu/eli/reg/2014/536/oj/eng
[20] Reis AA, Upshur R, Moodley K. Future-Proofing Research Ethics-Key Revisions of the Declaration of Helsinki 2024. JAMA. 2025 Jan;333(1):20-21. DOI: 10.1001/jama.2024.22254
[21] Bibbins-Domingo K, Brubaker L, Curfman G. The 2024 Revision to the Declaration of Helsinki: Modern Ethics for Medical Research. JAMA. 2025 Jan;333(1):30-31. DOI: 10.1001/jama.2024.22530
[22] Adams J. Defending explicability as a principle for the ethics of artificial intelligence in medicine. Med Health Care Philos. 2023 Dec;26(4):615-623. DOI: 10.1007/s11019-023-10175-7
[23] Ursin F, Timmermann C, Steger F. Explicability of artificial intelligence in radiology: Is a fifth bioethical principle conceptually necessary? Bioethics. 2022 Feb;36(2):143-153. DOI: 10.1111/bioe.12918
[24] Freyer N, Groß D, Lipprandt M. The ethical requirement of explainability for AI-DSS in healthcare: a systematic review of reasons. BMC Med Ethics. 2024 Oct;25(1):104. DOI: 10.1186/s12910-024-01103-2
[25] Morley J, Machado CCV, Burr C, Cowls J, Joshi I, Taddeo M, Floridi L. The ethics of AI in health care: A mapping review. Soc Sci Med. 2020 Sep;260:113172. DOI: 10.1016/j.socscimed.2020.113172
[26] Kempt H, Nagel SK. Responsibility, second opinions and peer-disagreement: ethical and epistemological challenges of using AI in clinical diagnostic contexts. J Med Ethics. 2022 Apr;48(4):222-229. DOI: 10.1136/medethics-2021-107440
[27] Bundesärztekammer, editor. Thesenpapier der Bundesärztekammer – Künstliche Intelligenz in der Gesundheitsversorgung. Deutscher Ärzteverlag; 2025. Available from: https://www.bundesaerztekammer.de/fileadmin/user_upload/BAEK/Themen/Digitalisierung/Thesenpapier_KI_in_der_Gesundheitsversorgung_03.2025.pdf
[28] Abbasi K. Declaration of Helsinki: a new revision at sixty years. J R Soc Med. 2024 Aug;117(8):255. DOI: 10.1177/01410768241284497
[29] Shaw JA. The Revised Declaration of Helsinki-Considerations for the Future of Artificial Intelligence in Health and Medical Research. JAMA. 2025 Jan;333(1):26-27. DOI: 10.1001/jama.2024.22074
[30] Ribeiro Junior HL. AI ethics in medical research: the 2024 Declaration of Helsinki. Lancet. 2024 Nov;404(10467):2048-2049. DOI: 10.1016/S0140-6736(24)02376-6
[31] Crootof R, Kaminski ME, Price II WN. Humans in the Loop. 76 Vanderbilt Law Review 429 (2023), U of Colorado Law Legal Studies Research Paper No. 22-10, U of Michigan Public Law Research Paper No. 22-011. SSRN; 2022. DOI: 10.2139/ssrn.4066781
[32] WMA – The World Medical Association. WMA Declaration of Taipei on Ethical Considerations regarding Health Databases and Biobanks. 2016 [cited 2025 Mar 4]. Available from: https://www.wma.net/policies-post/wma-declaration-of-taipei-on-ethical-considerations-regarding-health-databases-and-biobanks/
[33] Federal Office of Public Health (FOPH). Regulation of human research in Switzerland. 2024 [cited 2025 Mar 4]. Available from: https://www.bag.admin.ch/bag/en/home/medizin-und-forschung/forschung-am-menschen/regelung-humanforschungsgesetz.html
[34] Nix HP, Weijer C, Brehaut JC, Forster D, Goldstein CE, Taljaard M. Informed consent in cluster randomised trials: a guide for the perplexed. BMJ Open. 2021 Sep;11(9):e054213. DOI: 10.1136/bmjopen-2021-054213
Attachments
| Attachment 1 | Appendices (mibe000301_Attachment1.pdf, application/pdf, 207.66 KBytes) |

