Analysis of the current situation and potential for improvement of newborn hearing screening in Germany under consideration of different birth settings
Romina Jasmin Frenzel 1,2Susan Arndt 2
Stefan Dietsche 1
Oda von Rahden 1
1 Jade University of Applied Sciences Oldenburg, Technology and Health for People, Oldenburg, Germany
2 Albert-Ludwigs-University Freiburg, Faculty of Medicine, Freiburg, Germany
Abstract
Research question and objective: The aim of this study was to analyse the processes and interdisciplinary cooperation in newborn hearing screening, particularly in inpatient, outpatient and out-of-hospital settings. The challenges and potential for improvement were identified.
Method: The study is based on qualitative expert interviews with professionals involved in screening from clinics, ENT practices, birth centres and tracking centres in order to record and evaluate the experiences and perceptions of the actors. The evaluation is carried out as part of a qualitative summarised content analysis according to Mayring (2022).
Results: The results of n=17 interviews show that the screening process is influenced by time constraints, staff shortages and coordination problems. Logistical challenges and inadequate interdisciplinary communication occur particularly in outpatient and non-clinical settings.
Conclusion: Optimised use of resources, regular training and better coordination between professionals could improve the efficiency and quality of screening and increase reliability in all birth settings.
Keywords
newborn hearing screening, needs analysis, care structures, birth settings
Introduction
Newborn hearing screening was introduced in 2009 as part of the standard care provided by the statutory health insurance funds [1]. The follow-up evaluation (2017/2018) shows a screening rate of 86.1%. There are considerable differences in the documented screening rates between the federal states, ranging from 29.5 to 99.7% (2018). Only 42.4% (2018) of all birthing centres achieved the required screening rate of over 95%. The nationwide refer rate is 6.0% (2018) [2]. Refer rate is the proportion of newborns that do not pass the initial OAE and/or AABR and are referred for repeated screening or diagnostic assessment. This differs from screening coverage (screening rate), which is the proportion of all live births who undergo a screening test. A higher refer rate at unchanged coverage may indicate suboptimal test conditions or protocol adherence, whereas low coverage reduces the absolute number of referrals despite an unchanged rate. Outpatient and out-of-hospital births pose a particular challenge due to the inconsistent procedures in the care process. An analysis of the processes therefore appears necessary.
Research questions
The aim of this thesis is to identify and analyse the processes involved in newborn hearing screening, taking into account the different birth settings (outpatient, inpatient, out-of-hospital). The focus is on the organisational framework conditions, the test procedures for initial and second testing after birth as well as the organisation of reporting and subsequent tracking in the event of a positive result. Particular attention is paid to the interdisciplinary cooperation of the actors involved, as it appears to have a noticeable influence on the screening process.
Based on this objective, the following key research questions arise for the qualitative survey:
- Which organisational framework conditions and processes of newborn hearing screening can be identified in clinical, outpatient and non-clinical settings?
- To what extent is an interdisciplinary exchange realised between the actors involved in the screening process, and how does this vary depending on the birth setting?
- How can existing processes and the quality of screening be prospectively optimised in order to reduce the number of unscreened and undocumented children?
Method
As part of the research project, n=18 semi-structured qualitative expert interviews are being conducted from December 2024 until approximately April 2025. The sampling is based on the concept of theoretical saturation [3]. Recruitment was based on a systematically developed sampling matrix with the aim of achieving a heterogeneous sample from different obstetric care settings (inpatient, outpatient, out-of-hospital) in the federal state of Lower Saxony. The professionals involved in the process of newborn hearing screening will be recruited, including midwives in the clinical-inpatient setting in the delivery room, midwives working in out-of-hospital obstetrics, midwives with a focus on postpartum care, specialists with a focus on gynaecology, medical assistants, nurses, medical-technical staff, audiologists, ENT audiology assistants. The composition of the sample is illustrated in Table 1 [Tab. 1].
Table 1: Sampling matrix of interviewees by birth setting, professional role and region type (preliminary)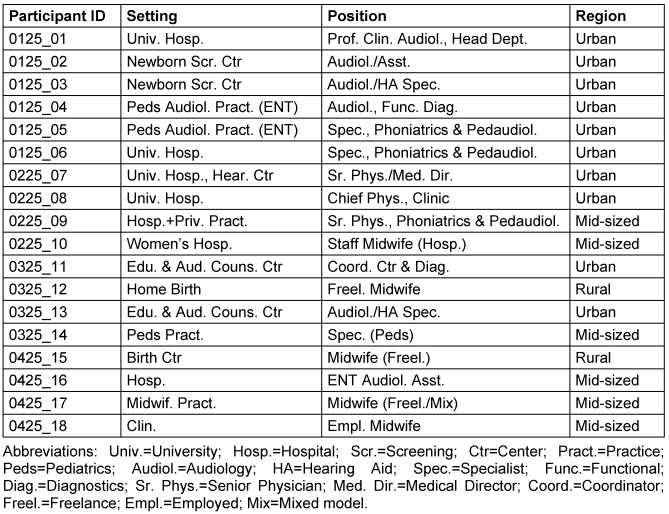
The data analysis is carried out as a summarising, inductive content analysis according to Mayring [4] using MAXQDA software. The results were analysed in parallel to the ongoing interview phase. Preliminary results are presented below with reference to the ongoing data collection phase.
Results
Results are based on the analysis of currently n=17 expert interviews. The content of the data is structured on the basis of a preliminary category system, which is developed iteratively and continuously reviewed in line with Mayring’s summarising content analysis [4]. Although the category system is still in the development process, the interviews analysed so far already allow us to derive initial analytically robust statements. In particular, recurring patterns can be identified with regard to structural framework conditions, procedural challenges and interdisciplinary collaboration within the various screening contexts. The current category system forms the basis for the final category development and will be fully reflected upon, summarised and validated based on theory once the data collection has been completed. First results are presented according to the main and sub-categories developed.
Process flows and process quality
Significant differences between the various birth settings were identified when analysing the newborn hearing screening processes. In the inpatient setting, screening is predominantly carried out as a standardised process, but time restrictions and personnel resources influence the procedure. One interviewee reported: ‘Screening is usually carried out directly on the first day after the birth, but we often have little time because the wards are full and we have many other tasks to complete’ (IP0125_01, Head of Audiology, clinic). This illustrates the challenges in the screening process, particularly with regard to time pressure and staff shortages. The availability of parents plays a central role in the outpatient setting. Coordination with the parents and access to resources are crucial here, which led to more irregularities in the process compared to the clinical setting. In the out-of-hospital setting, especially for home births, coordination between birth centres (out-of-hospital facilities) and doctors poses a challenge. One interviewee explained:
Spatial and infrastructural conditions lead to a delay in screening and increase uncertainty in the process. The newborn hearing screening processes in the various settings are characterised by temporal, organisational and logistical challenges. These findings underline the need for improved coordination, more flexible resource allocation and optimised scheduling in order to ensure the quality of screening in all birth settings.
Interdisciplinarity
The analysis of the interviews shows that in several cases there is insufficient cooperation and limited communication between the different actors, which potentially impairs the screening process. In the out-of-hospital setting, particularly in the case of home births and collaboration with midwives, it was often found that there is no regular communication between the midwives and medical professionals. A specialist from the phoniatrics and paediatric audiology department of a clinic reported:
This statement refers to the lack of structured communication between the midwives and the medical specialists, which makes it difficult to pass on relevant information, such as abnormalities during labour or the need for further examination. Problems in coordination between clinics and general practitioner (GP) practices were also identified in the clinical setting, where staff shortages and inadequate communication meant that important information about the status of the newborn was not passed on, which can lead to delays in screening (IP0225_09, specialist, clinic).
Problem areas and challenges
In the inpatient setting, time pressure and staff shortages lead to delays in the screening process, especially if other tasks interfere with the test being carried out. One interviewee reported:
In the outpatient setting, the availability of appointments and coordination with parents are particularly crucial. Screening is often delayed due to late appointments or a lack of resources. In the out-of-hospital setting, particularly in the case of home births, spatial and infrastructural restrictions as well as coordination between birthing centres and specialists are problematic, which makes it more difficult to carry out the test. In addition, there are frequent communication gaps between the institutions involved, which leads to incomplete documentation and incorrect tracking of screening results. Technical problems with equipment and a lack of specialised staff and regular training also make it difficult to carry out the screening. These challenges highlight the need for better coordination, resource planning and more flexible organisation in order to increase the efficiency and quality of screening.
Potential for improvement
The needs analysis shows several areas for improvement in the areas of resource management, staff training, coordination and technical equipment. A lack of technology and staff shortages were identified as frequent problems that delay the screening process, particularly in out-of-hospital settings. A key improvement is the training of staff in order to improve communication with parents. A midwife from the out-of-hospital sector comments:
This statement emphasises the need for regular training to promote knowledge about the screening process and to educate parents. It also shows that better coordination between the professionals from the different birth settings, especially between midwives, doctors and audiological staff, could increase the efficiency of the screening.
Conclusion
The results of the needs analysis make it clear that the process of newborn hearing screening in the various birth settings is noticeably influenced by time restrictions, insufficient interdisciplinary cooperation and logistical and organisational challenges. These structural and process-related framework conditions have an impact on the quality and efficiency of screening and highlight the need for action. Improved coordination, flexible resource planning and optimised scheduling are essential to ensure and further develop the quality of care. In addition, targeted training measures for the specialist staff involved and more effective utilisation of resources offer relevant potential for process improvement. Consistent implementation of these measures can make an important contribution to sustainable quality assurance and to strengthening the reliability of care in newborn hearing screening.
Notes
Conference presentation
This contribution was presented at the 27th Annual Conference of the German Society of Audiology and published as an abstract [5].
Competing interests
The authors declare that they have no competing interests.
References
[1] Gemeinsamer Bundesauschuss. Neugeborenen-Hörscreening. Zusammenfassende Dokumentation zum Normsetzungsverfahren. 2008 [last accessed 2024 Nov 11]. Available from: https://www.g-ba.de/downloads/40-268-759/2008-12-17-Abschluss-H%C3%B6rscreening.pdf[2] Brockow I, Söhl K, Hanauer M, Heißenhuber A, Marzi C, Am Zehnhoff-Dinnesen A, Matulat P, Mansmann U, Nennstiel U. Neugeborenen-Hörscreening in Deutschland – Ergebnisse der Evaluationen 2011/2012 und 2017/2018 [Newborn hearing screening in Germany-results of the 2011/2012 and 2017/2018 evaluations]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2023 Nov;66(11):1259-67. DOI: 10.1007/s00103-023-03779-0
[3] Corbin J, Strauss A. Grounded Theory: Grundlagen Qualitativer Sozialforschung. 1st ed. Weinheim/Basel: Beltz; 1990.
[4] Mayring P. Qualitative Inhaltsanalyse. Grundlagen und Techniken. 13th ed. Weinheim/Basel: Beltz; 2022.
[5] Frenzel RJ, Arndt S, Dietsche S, von Rahden O. Analyse der Ist-Situation und Verbesserungspotenziale des Neugeborenenhörscreenings in Deutschland unter Berücksichtigung verschiedener Geburtssettings. In: Deutsche Gesellschaft für Audiologie e. V.; ADANO, editors. 27. Jahrestagung der Deutschen Gesellschaft für Audiologie und Arbeitstagung der Arbeitsgemeinschaft Deutschsprachiger Audiologen, Neuroontologen und Otologen. Göttingen, 19.-21.03.2025. Düsseldorf: German Medical Science GMS Publishing House; 2025. Doc213. DOI: 10.3205/25dga213

