[Arbeitszufriedenheit von Hebammen im klinischen Setting: Eine Querschnittserhebung in Deutschland]
Sonja Wangler 1,2Gabriele Meyer 1
Gertrud M. Ayerle 1
1 Institute of Health and Nursing Science, Medical Faculty, Martin Luther University Halle-Wittenberg, Halle (Saale), Germany
2 School of Health Sciences and Management, Baden-Wuerttemberg Cooperative State University (DHBW), Stuttgart, Germany
Zusammenfassung
Hintergrund: Arbeitszufriedenheit (AZ) wirkt sich auf die Arbeitsleistung, das persönliche Wohlbefinden und den Verbleib im Beruf aus. Das Arbeitsumfeld beeinflusst die AZ, wobei die Gestaltung des Gebärraums auf die Handlungspraxis von Hebammen und ihre Zufriedenheit noch wenig untersucht ist. Ziel ist es, die AZ von Hebammen im klinischen Setting und die Zufriedenheit mit der Gestaltung des Gebärraums zu untersuchen und Zusammenhänge zu beschreiben.
Methode: Es wurde eine Online-Querschnittserhebung durchgeführt. Die Stichprobe bestand aus Hebammen (N=323), die in der klinischen Geburtshilfe in Deutschland arbeiten. Die Daten wurden deskriptiv ausgewertet und mit statistischen Analyseverfahren untersucht.
Ergebnisse: Die globale AZ lag ebenso im mittleren Bereich wie die Zufriedenheit mit der Raumgestaltung. Am unzufriedensten waren die Hebammen mit der Zeit, die ihnen für die Betreuung von Frauen zur Verfügung stand und mit ihrem Gehalt. Die Zufriedenheit mit dem Team war hoch und war zusammen mit der Unterbesetzung der größte Einflussfaktor auf die globale AZ. Die Zufriedenheit mit der Raumgestaltung hatte nur einen geringen Einfluss auf die AZ.
Schlussfolgerung: Die Studie zeigt auf, dass die AZ durch Förderung des Teams und eine ausreichende Personalbesetzung gesteigert werden kann. Der Zusammenhang von Gebärumgebung, Betreuungsmodell und Arbeitszufriedenheit von Hebammen bedarf weiterer Untersuchung.
Schlüsselwörter
Arbeitszufriedenheit, Hebammen, klinisches Setting, Gebärraumgestaltung, Querschnittserhebung
Background
In Germany, around 98% of all children are born in hospital [27], where midwives are usually the first point of contact for expectant mothers. In order to be able to provide high-quality and safe midwifery care, adequate staffing is of the essence. In recent years, midwives have reported an increasing workload and declining working conditions resulting from factors such as staff shortages, bureaucratic and administrative requirements, and the increasing medicalisation and technicisation of midwifery [1], [24]. These conditions have a negative impact on the job satisfaction of midwives in a hospital setting, increasing their intention to change jobs or leave midwifery entirely [1], [2], [5]. In order to counter this development, studies are needed to explore the variety of factors influencing job satisfaction and to identify approaches that can positively influence the job satisfaction and retention of hospital midwives.
Staff satisfaction contributes to the overall performance and success of organisations and has an impact on staff commitment and retention [23]. The construct of job satisfaction includes different aspects such as work content and the associated requirements and duties, the social importance of the job and the prospects for professional development. Relationships in the workplace, including teamwork, support from colleagues and managers, work organisation, working hours, the work environment and safety in the workplace all play a role in this concept [23], [26]. Previous research addressing midwives’ job satisfaction has identified the following influencing factors: Along with good teamwork, positive relationships with colleagues and appreciation and support from managers [5], [22], professional autonomy, the importance of the job, development potential, the relationship with the women being cared for, and opportunities to support natural labour can all contribute to job satisfaction [5], [13], [42]. Factors that lead to a decrease in job satisfaction, on the other hand, are high workload, staff and resource shortages, conflicts when it comes to reconciling work and family life, as well as a low salary [1], [20], [24], [29], [36].
The physical work environment and its influence on work performance and job satisfaction has only recently become the focus of research [11], [12], [32], [40].
The physical work environment refers to all material objects and stimuli in the workplace [34]. Models for studying stress in the workplace, in particular, place a focus on the physical work environment or workplace conditions [40]. A pleasant physical work environment can improve job satisfaction, whereas an unpleasant work environment can have a negative impact on job satisfaction [12]. Employees have a stronger sense of attachment to their place of employment if they can identify with their work environment and perceive it as both attractive and functional in terms of the work tasks and activities to be performed [40].
To date, findings regarding the influence of the physical work environment on midwives’ job satisfaction are scarce. The assessment of the work environment reveals that, on the one hand, the delivery rooms in the department and, on the other, the number/set-up of break rooms or social areas, as well as the offices and changing rooms all play an important role [1], [39]. The delivery rooms themselves, referred to in this text as birthing rooms to distinguish between them and the labour ward, influence the working practice of midwives with their design and set-up [18], [19], [28]. Hospital birthing rooms are characterised by a technicised and risk-oriented view of obstetrics [7], [35]. This is reflected in their design and set-up [3], [21]. Midwives describe the importance of the atmosphere and the set-up of the birthing room in promoting a physiological birth. As central aspects here, the midwives mentioned peace and quiet as well as intimacy for the birthing women, the promotion of upright positions during labour and the removal of the bed from the centre of the room [6], [8], [9]. Midwives who work in both a homebirth and a hospital setting report being stressed by the clinical rooms in the hospital [6], [9]. Studies investigating a redesign of birthing rooms identified positive outcomes for the birthing women themselves as well as increased staff satisfaction with the rooms and a reduced stress level [3], [14], [28]. These findings lead us to expect an impact on job satisfaction.
Against this background, the current study addresses the question of how satisfied midwives in the hospital setting in Germany are with the design of the birthing rooms and what impact the room design has on job satisfaction. The aim is to (1) collect data on the job satisfaction of midwives in a hospital setting as well as their satisfaction with the design of the birthing room, (2) to explore correlations/factors influencing the different dimensions of work satisfaction, and (3) to investigate the influence of selected socio-demographic variables.
Methodology
The study comprises a cross-sectional survey using a validated questionnaire [37].
Study context and participants
The survey is embedded in the “Be-Up: Geburt aktiv” multicentre randomised controlled trial (RCT). From 2017 to 2021, in a total of 22 hospitals across Germany, one delivery room was redesigned to create an “alternative” Be-Up birthing room with the aim of promoting natural labour in the hospital. In the Be-Up birthing room, the delivery bed was removed from the centre of the room (or concealed), active movement, upright positions and self-determination of the woman during contractions were all encouraged using various different elements (floor mat, foam cubes, birthing stool), and a monitor showing nature films supported relaxation. There was also a table and a set of chairs along with a snack bar and dimmable light [4].
We surveyed midwives in Germany who, at the time of the survey, were working in the labour ward. The study was based on a convenience sample, which we partly obtained through the hospitals participating in the Be-Up trial and partly by means of targeted snowball sampling. In a first analysis, the midwives who participated in the Be-Up study were compared with midwives working in other hospitals to assess the effects of the new room design [41]. The object of the study reported here is data from the total sample, comprising midwives participating in the Be-Up trial and midwives from other hospitals across Germany.
Data collection
The data collection was conducted in March and April 2021 via online questionnaires using the SoSci Survey software [25]. The questionnaire was distributed in Be-Up hospitals, firstly using a poster with a QR code that was displayed in the midwives’ break room and secondly via contact persons in the Be-Up hospitals who emailed the link for the questionnaire to all midwives. In order to also access those midwives working in the typical birthing rooms, the invitation to participate in the questionnaire was sent out via the German Midwifery Association’s “hospital-employed midwives” mailing list and their “labour ward management” mailing list. In addition to this, the Chairs of the Federal State Midwifery Associations were also asked to distribute the questionnaire to their members by email. Some of the regional associations also printed the QR code in their newsletters, and the German Society for Midwifery Science (DGHWi) did the same on their website. In one federal state, the hospitals were contacted directly in writing as part of an information mailing conducted by the midwifery association. In addition, we used social media, in the form of Facebook, and asked people to pass the information on.
Variables and measurement instrument
The validated questionnaire “Job satisfaction and room design among midwives” (Arbeitszufriedenheit- und Raumgestaltung Hebammen, ARaH) included, along with items on global job satisfaction, the following dimensions of the construct of job satisfaction: team, autonomy and development potential. The items on birthing room design and set-up were generated via a qualitative pre-study and the other items were created using a scoping review [37]. The different dimensions each comprise between 4 and 14 items reflecting different aspects of the construct. Moreover, the questionnaire includes items from the Job Satisfaction Scale [43] which was developed and validated by Warr et al. and now also exists in German translation [16]. Responses were given on a 7-point interval scale with labels only on the endpoints, where 7 represented the highest level of satisfaction in each case. The questionnaire included one item regarding the respondent’s overall health on a 5-point scale, where 5 represented the best state of health. The items on the room set-up dimension were dichotomous. The following socio-demographic data was collected in the questionnaire: age, gender, professional experience, scope of employment, the hospital level of care, and prevalence of understaffed shifts. In Germany, obstetric departments are classified into four levels of care. Level one perinatal centres offer the highest standard of care and include a Neonatology Department equipped to manage preterm and critically ill neonates (Neonatal Intensive Care Unit). In contrast, level four represents maternity units without in-house paediatricians (birth centres with basic care).
Ethical considerations
The survey was conducted anonymously with consent being given by completing the questionnaire. The Ethics Committee of the Faculty of Medicine at Martin-Luther-Universität Halle-Wittenberg voted positively on this study (case number 2019-131 (B)).
Statistical analysis
The analysis of the data was conducted using the statistical program SPSS (version 27).
To describe the sample, frequencies and percentages as well as means (standard deviation) for the metric variables were calculated for the categorial data. A mean value was also calculated for the individual dimensions. Negatively formulated questions were reversed for analysis. To determine the internal consistency of the scales, Cronbach’s Alpha was calculated. A multiple linear regression analysis was used to explore what correlations exist between the different variables of room design, team and autonomy (independent variables), as well as global job satisfaction (dependent variable). The hospital level of care and understaffing were also included in the regression analysis. The data was tested for normal distribution. Depending on the distribution of the data, either parametric tests (T-tests) or non-parametric tests (Mann Whitney U-tests) were performed. Missing values were excluded in pairs.
A p-value of .05 or less was defined as statistically significant. A reliability analysis was also performed.
Results
A total of 367 datasets were exported to SPSS; n=44 incomplete questionnaires were excluded, leaving us with a sample of 323 responses from midwives.
Socio-demographics
The average age was 38.4 (SD 11.3) with a minimum age of 20 and a maximum of 62. The average length of professional experience was 15.0 years (SD 11.5). A total of 79.3% (n=256) of the midwives were directly employed by a hospital, 8% (n=26) worked as hospital-affiliated freelance midwives (Belegsystem) and 19.8% (n=64) worked as freelancers alongside their salaried positions. Overall, 57% (n=184) of the midwives worked part-time, 31.3% (n=101) worked full-time. A total of 40.6% (n=131) worked in a level one perinatal centre, 8% (n=26) in a level two hospital, 3.1% (n=10) in a hospital with a perinatal specialism and 35.6% (n=115) in a maternity hospital with no specialism (basic care).
A total of 33.7% (n=109) of the midwives reported that their department was often understaffed, 31.6% (n=102) reported rare understaffing, 4.6% (n=15) of the midwives reported that their departments were always understaffed, and 12.1% (n=39) said this never happened. A total of 18% (n=58) did not respond to this question.
The internal consistency of the different dimensions in the questionnaire was good with a Cronbach’s Alpha of 0.769–0.920.
(1) Job satisfaction and satisfaction with room design
The satisfaction values (mean values and standard deviations) of the scales or the individual items in the room design dimension and of the Job Satisfaction Scale are displayed in Table 1 [Tab. 1].
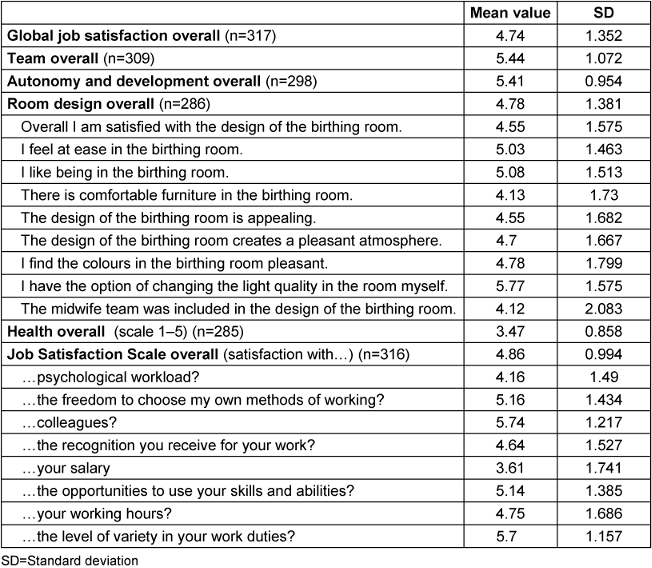
Based on the mean values of the scales, satisfaction with the team scored highest (5.44) and room design scored lowest (4.78). In the analysis of the individual items, satisfaction with salary and the time available to properly care for the women showed the lowest values (3.61 and 3.99, respectively), while the items “team members help one another” and “I have the skills I need to work in the birthing room” had the highest satisfaction scores, each with a mean value of 6.11.
Figure 1 [Fig. 1] shows the set-up of the birthing rooms.
Figure 1: Set-up of birthing room (n=323)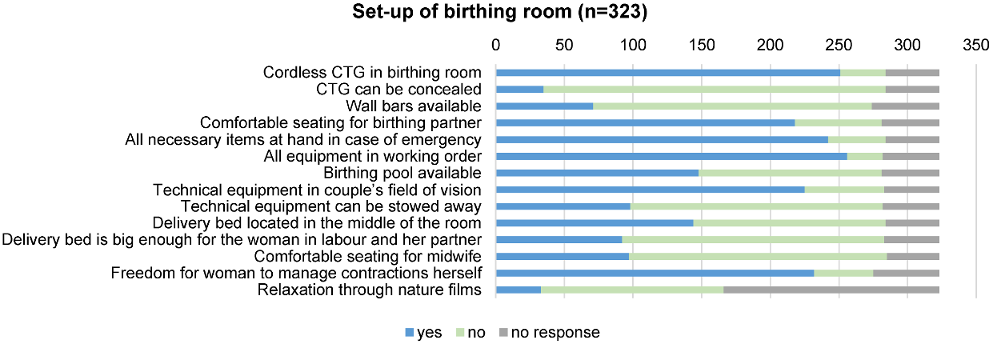
(2) Correlations between the dimensions of job satisfaction
The multiple linear regression analysis (see Table 2 [Tab. 2]) showed that the satisfaction with the team, understaffing and state of health had a significant impact on global job satisfaction, F (7.24)=37.69 p<0.001. (If understaffing increases by one point, job satisfaction falls by 0.6 points; if the team is rated one point better, job satisfaction increases by 0.5 points). Autonomy and room design, however, had a low impact on global job satisfaction. The model had a high goodness of fit with a corrected R-squared value of 0.51.
Table 2: Regression analysis (n=251)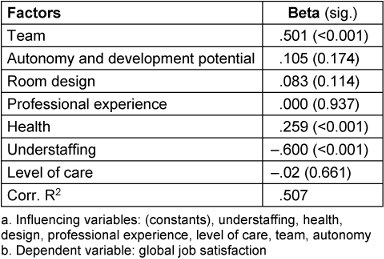
To analyse the lower and upper extremes of job satisfaction, the group of midwives with very high job satisfaction (n=77) was compared with the group of midwives with very low job satisfaction (n=52). Very low job satisfaction was defined as having a score of between 1 and 3 for global job satisfaction and very high as having a score of 6 to 7.
In the team (U=453.00, Z=–7.13, p<0.001), autonomy (U=586.00, Z=–5.91, p<0.001), room design (U=654.50, Z=–5.28, p<0.001) and health (U=1,061.50, Z=–2.86, p=0.004) dimensions, the Mann Whitney U-tests yielded significantly higher values in the group with higher job satisfaction.
(3) Correlations between socio-demographic variables and job satisfaction
Age and professional experience had no impact on job satisfaction. Even in the comparison of the extremes at either end of the job satisfaction scale, there was no significant difference with regard to professional experience (U=1,163.00, z=–1.45, p=0.148). The midwives in the group with the low job satisfaction were significantly more likely to be working for a hospital providing the maximum level of care (level one) (U=1,164.50, Z=–2.36, p=0.019) and their departments significantly more frequently understaffed (U=302.00, Z=–7.15, p<0.001). The comparison of midwives in full-time and part-time employment showed no significant differences between the two.
Correlations with the hospital level of care
The comparison of midwives from level one hospitals (highest care level) (n=131) with those from maternity hospitals without a perinatal specialism (birth centre with basic care) (n=114) is displayed in Figure 2 [Fig. 2].
Figure 2: Comparison of level one perinatal centre (highest care level in Germany) and maternity hospital without perinatal specialism (basic care) (mean values of the group)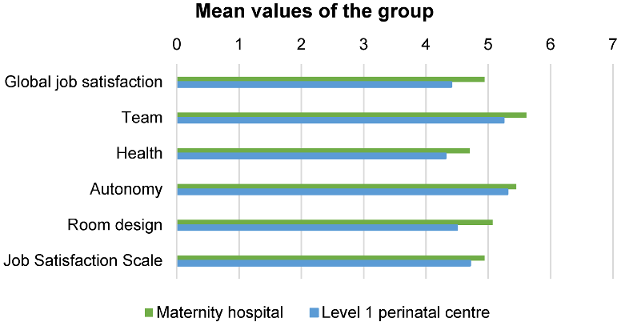
There was a statistically significant difference in global job satisfaction (t(243)=–3.00, p=0.03), with midwives in maternity hospitals being more satisfied (M=4.91, SD=1.33) than midwives in level one hospitals (M=4.41, SD=1.40). They more frequently reported (t(243)=–3.56, p<0.001) having sufficient time to properly look after the women in their care (M=4.34, SD=1.61) than the midwives in the level one perinatal centres (M=3.53, SD=1.60). The satisfaction with the team (level one: M=5.25, SD=1.14 maternity hospitals: M=5.61, SD=1.09) was also higher in this group (t(243)=–2.54, p=0.01). There was no statistically significant difference when it came to autonomy and state of health. The midwives in the maternity hospitals were significantly more satisfied, especially with the design of the birthing room (t(242)=–3.35, p<0.001). The midwives from the level one hospitals had slightly less professional experience and were younger (professional experience: level one: M=13.19, SD=11.02, maternity hospitals: M=16.03, SD=11.14, p=0.051; age: level one: M=36.21, SD=10.73; maternity hospitals: M=39.53, SD=11.23, p=0.021).
Discussion
The aim of the study was to assess the current state of research on the job satisfaction of midwives in hospital settings, especially on aspects of the work environment and room design in correlation with selected socio-demographic variables.
The study participants predominantly scored global job satisfaction and the individual dimensions of job satisfaction in the middle range. In an international comparison, too, [30], [33] midwives job satisfaction is often only in the middle range. In the nationwide study on in-hospital midwifery care by Albrecht et al., only around 50% of midwives in Germany reported that they would choose the same profession again and 39% were dissatisfied with the overall working conditions [1]. The midwives in the study also stated that their working conditions had deteriorated in recent years and they had to care for more women at the same time. Dissatisfaction with the time available to care for women in the delivery room was evident in the present study and is in stark contradiction to the calls for 1:1 care and to the positive outcomes this has for both mother and child [10]. The relationship between the woman in labour and the midwife is one of the factors impacting job satisfaction [38]. The more women midwives have to care for at the same time, the greater their intention to change professions [1], [36]. Rodriguez et al. established a link between the assessment of the work environment, the safety of the mother and child, and the intention to change professions [33].
In the present study, satisfaction with the design of birthing rooms was only moderate. Certain aspects of the room set-up were identified which could have had a negative impact on both the birthing mother and the midwife. These included technical equipment which could not be stowed away and were in the couple’s field of vision, a delivery bed which was positioned in the middle of the room and was not big enough for the woman in labour and her birth partner, as well as a lack of comfortable seating for the midwife. The aspects described here could prevent midwives from promoting physiological birth [3], [28], [35]. The expert report on midwifery care in Germany showed that 20% of midwives were dissatisfied with the set-up of the birthing rooms [1]. By changing the birthing environment to one facilitating natural labour, studies showed that a higher level of satisfaction with the birthing rooms could be achieved, with the atmosphere in the rooms being highlighted as a particularly positive factor here [15], [28]. These studies also showed that the design of a room is closely associated with the model of care or the approach to care and redesigning the room brings a change in the perspective of the caregiver from a risk and technology-oriented perspective to a salutogenetic and woman-centred one [3], [15].
Midwives’ dissatisfaction with their salary shown by this study also corresponds to the findings of the study conducted by Albrecht et al., as well as other studies both in Germany and internationally [1], [24], [29], and provides policymakers with an opportunity to increase midwives’ satisfaction by offering appropriate remuneration.
The present study identified the team, the frequency of understaffed shifts and health as the most important factors influencing midwives’ job satisfaction. This is confirmed by the findings of previous studies, which showed that relationships and team support in the workplace were important predictors for midwives’ job satisfaction [5], [22], [29]. From this we can derive that there is a need to strengthen the team through appropriate measures.
For midwifery practice, it is particularly important that the negative impact of understaffing and increased workload on midwives’ satisfaction is given more political attention and efforts are made to counter it, as this has a demonstrable effect on midwives’ intention to leave the profession, which exacerbates the problem [1], [17], [29], [31].
The correlation observed between state of health and job satisfaction is also confirmed by the literature [24]. Some studies show a correlation between dissatisfaction in the workplace and health effects in the form of sick days or even burnout [24], [29].
The higher level of satisfaction that this study found among midwives working in maternity hospitals without a perinatal specialism compared to midwives working in level one hospitals (highest care level) requires further investigation. In the level one hospitals, midwives experienced more understaffed shifts and had less time to look after the women in their care. The higher number of births (an average of around 2,000 per year compared to an average of 800 for the level four hospitals) [1] along with the higher rate of pathological births in level one hospitals could result in increased work demands. Besides these increased demands, the more difficult conditions faced by the midwives in promoting physiological births could also have a negative impact on their job satisfaction [14], [19], [28]. In smaller hospitals, midwives were more satisfied with their teams which could testify to better cohesion in a smaller team.
Limitations
Recruitment was carried out using snowball sampling and to some extent also the German Midwifery Association’s mailing lists, which posed the problem that not all hospital-based midwives are members of the association. Due to the sampling method, it is impossible to say how many midwives had access to the questionnaire and the response rate can therefore not be determined. Nor do we know the regional distribution of the sample. It could be the case that certain hospitals had a disproportionate number of participants, whereas others had none. Nevertheless, our sample reflects the sample used in the expert report on in-hospital midwifery care in terms of age structure, professional experience, the scope of employment of midwives and their distribution over the four different levels of hospital care [1].
Another limitation of this survey is that part of the sample (n=84) also took part in the “Be-Up: Geburt aktiv” study, which could have influenced the job satisfaction or response behaviour regarding the room design. One difficulty with a survey on the design of birthing rooms is that birthing rooms within one department can have different designs. The midwives in this study were therefore asked about only one birthing room, either the “Be-Up” room or the room in which they prefer to look after the women in their care. This may, on the one hand, have positively inflated the assessment of the room, but, on the other, it is possible that the effects of the birthing room were assessed in a more nuanced way compared to the sweeping assessment of all the birthing rooms in a department.
The cross-sectional design of the study meant only correlations could be shown, but no causal influencing factors. Moreover, our survey was conducted in the middle of the Covid-19 pandemic which changed the working conditions for midwives in a hospital setting.
Conclusions
The current study underlines existing evidence regarding the promotion of job satisfaction among midwives in a hospital setting, which can be achieved by strengthening the team and collaboration. The study emphasises, in particular, the need to tackle understaffing and also highlights the midwives’ dissatisfaction with the time they have available to look after the women in their care. The findings on room design and set-up revealed approaches to better aligning the birthing space with the needs of the birthing woman and the midwife, thus increasing satisfaction with the work environment. The correlation between the physical work environment, the model of care and the job satisfaction of midwives requires further investigation.
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Albrecht M, Loos S, Heiden an der I, Temizdemir E, Ochmann R, Sander M, Bock H. Stationäre Hebammenversorgung. 2019 [accessed 2025 Nov 17]. Available from: https://www.iges.com/sites/iges.de/myzms/content/e6/e1621/e10211/e24893/e24894/e24895/e24897/attr_objs24976/IGES_stationaere_Hebammenversorgung_092019_ger.pdf[2] Alnuaimi K, Ali R, Al-Younis N. Job satisfaction, work environment and intent to stay of Jordanian midwives. Int Nurs Rev. 2020 Sep;67(3):403-10. DOI: 10.1111/inr.12605
[3] Andrén A, Begley C, Dahlberg H, Berg M. The birthing room and its influence on the promotion of a normal physiological childbirth - a qualitative interview study with midwives in Sweden. Int J Qual Stud Health Well-being. 2021 Dec;16(1):1939937. DOI: 10.1080/17482631.2021.1939937
[4] Ayerle GM, Schäfers R, Mattern E, Striebich S, Haastert B, Vomhof M, Icks A, Ronniger Y, Seliger G. Effects of the birthing room environment on vaginal births and client-centred outcomes for women at term planning a vaginal birth: BE-UP, a multicentre randomised controlled trial. Trials. 2018 Nov;19(1):641. DOI: 10.1186/s13063-018-2979-7
[5] Bloxsome D, Ireson D, Doleman G, Bayes S. Factors associated with midwives' job satisfaction and intention to stay in the profession: An integrative review. J Clin Nurs. 2019 Feb;28(3-4):386-99. DOI: 10.1111/jocn.14651
[6] Bourgeault IL, Sutherns R, Macdonald M, Luce J. Problematising public and private work spaces: midwives' work in hospitals and in homes. Midwifery. 2012 Oct;28(5):582-90. DOI: 10.1016/j.midw.2012.06.002
[7] Bowden C, Sheehan A, Foureur M. Birth room images: what they tell us about childbirth. A discourse analysis of birth rooms in developed countries. Midwifery. 2016 Apr;35:71-7. DOI: 10.1016/j.midw.2016.02.003
[8] Carolan-Olah M, Kruger G, Garvey-Graham A. Midwives' experiences of the factors that facilitate normal birth among low risk women at a public hospital in Australia. Midwifery. 2015 Jan;31(1):112-21. DOI: 10.1016/j.midw.2014.07.003
[9] Davis DL, Homer CS. Birthplace as the midwife's work place: How does place of birth impact on midwives? Women Birth. 2016 Oct;29(5):407-15. DOI: 10.1016/j.wombi.2016.02.004
[10] Deutsche Gesellschaft für Gynäkologie und Geburtshilfe (DGGG); Deutsche Gesellschaft für Hebammenwissenschaft (DGHWi). S3-Leitlinie: Die vaginale Geburt am Termin. Registernummer 015-083. AWMF; 2020 [accessed 2025 Nov 17]. Available from: https://register.awmf.org/de/leitlinien/detail/015-083
[11] Djukic M, Kovner C, Budin WC, Norman R. Physical work environment: testing an expanded model of job satisfaction in a sample of registered nurses. Nurs Res. 2010;59(6):441-51. DOI: 10.1097/NNR.0b013e3181fb2f25
[12] Djukic M, Kovner CT, Brewer CS, Fatehi F, Greene WH. Exploring direct and indirect influences of physical work environment on job satisfaction for early-career registered nurses employed in hospitals. Res Nurs Health. 2014 Aug;37(4):312-25. DOI: 10.1002/nur.21606
[13] Edmondson MC, Walker SB. Working in caseload midwifery care: the experience of midwives working in a birth centre in North Queensland. Women Birth. 2014 Mar;27(1):31-6. DOI: 10.1016/j.wombi.2013.09.003
[14] Foureur M, Davis D, Fenwick J, Leap N, Iedema R, Forbes I, Homer CS. The relationship between birth unit design and safe, satisfying birth: developing a hypothetical model. Midwifery. 2010 Oct;26(5):520-5. DOI: 10.1016/j.midw.2010.05.015
[15] Goldkuhl L, Tistad M, Gyllensten H, Berg M. Implementing a new birthing room design: a qualitative study with a care provider perspective. BMC Health Serv Res. 2023 Oct;23(1):1122. DOI: 10.1186/s12913-023-10051-3
[16] Götz K, Broge B, Willms S, Joos S, Szecsenyi J. Die Arbeitszufriedenheit von Allgemeinmedizinern [Job satisfaction of general practitioners]. Med Klin (Munich). 2010 Nov;105(11):767-71. DOI: 10.1007/s00063-010-8881-z
[17] Grylka-Baeschlin S, Aeberli R, Guenthard-Uhl B, Meier-Kaeppeli B, Leu-Tenegger V, Volken T, Pehlke-Milde J. Job satisfaction of midwives working in a labor ward: A repeat measure mixed-methods study. Eur J Midwifery. 2022;6:8. DOI: 10.18332/ejm/145494
[18] Hammond A, Foureur M, Homer CS. The hardware and software implications of hospital birth room design: a midwifery perspective. Midwifery. 2014 Jul;30(7):825-30. DOI: 10.1016/j.midw.2013.07.013
[19] Hammond A, Homer CSE, Foureur M. Friendliness, functionality and freedom: Design characteristics that support midwifery practice in the hospital setting. Midwifery. 2017 Jul;50:133-8. DOI: 10.1016/j.midw.2017.03.025
[20] Hansson M, Dencker A, Lundgren I, Carlsson IM, Eriksson M, Hensing G. Job satisfaction in midwives and its association with organisational and psychosocial factors at work: a nation-wide, cross-sectional study. BMC Health Serv Res. 2022 Apr;22(1):436. DOI: 10.1186/s12913-022-07852-3
[21] Hodnett ED, Stremler R, Weston JA, McKeever P. Re-conceptualizing the hospital labor room: the PLACE (pregnant and laboring in an ambient clinical environment) pilot trial. Birth. 2009 Jun;36(2):159-66. DOI: 10.1111/j.1523-536X.2009.00311.x
[22] Jasiński AM, Derbis R. Social support at work and job satisfaction among midwives: The mediating role of positive affect and work engagement. J Adv Nurs. 2023 Jan;79(1):149-60. DOI: 10.1111/jan.15462
[23] Judge TA, Zhang SC, Glerum DR. Job satisfaction. In: Sessa VI, Bowling NA, editors. Essentials of job attitudes and other workplace psychological constructs. New York: Routledge; 2020. p. 207-41.
[24] Kohler S, Bärnighausen T, Eichenauer J, Scheichenbauer C, Paul N. Gesundheit und berufliche Zufriedenheit von freiberuflichen und angestellten Hebammen: Ergebnisse einer Hebammenbefragung in Baden-Württemberg [Health and Professional Satisfaction of Freelance and Employed Midwives: Results of a Survey of Midwives in Baden-Wuerttemberg]. Gesundheitswesen. 2023 May;85(5):e5-e15. DOI: 10.1055/a-1851-9619
[25] Leiner DJ. SoSci survey. 2014; [accessed 2025 Nov 17]. Available from: https://www.soscisurvey.de
[26] Locke EA. The nature and causes of job satisfaction. In: Dunnette MD, editor. Handbook of industrial and organizational psychology. Chicago: Rand McNally; 1976. p. 1297-343.
[27] Loytved C. Qualitätsbericht 2021 – Außerklinische Geburtshilfe in Deutschland. Gesellschaft für Qualität in der außerklinischen Geburtshilfe e.V. (QUAG e.V.); 2022 [accessed 2025 Nov 17]. Available from: https://www.quag.de/downloads/QUAG_Bericht2021.pdf
[28] Murray-Davis B, Grenier LN, Plett RA, Mattison CA, Ahmed M, Malott AM, Cameron C, Hutton EK, Darling EK. Making Space for Midwifery in a Hospital: Exploring the Built Birth Environment of Canada's First Alongside Midwifery Unit. HERD. 2023 Apr;16(2):189-207. DOI: 10.1177/19375867221137099
[29] Nedvedova D, Dvaov B, Jarosova D. Job Satisfaction of midwives: a literature review. Cent Eur J Nurs Midw. 2017;8(2):650-6. DOI: 10.15452/CEJNM.2017.08.0014
[30] Papoutsis D, Labiris G, Niakas D. Midwives’ job satisfaction and its main determinants: A survey of midwifery practice in Greece. Br J Midwifery. 2014;22(7):480-6. DOI: 10.12968/bjom.2014.22.7.480
[31] Peter KA, Meier-Kaeppeli B, Pehlke-Milde J, Grylka-Baeschlin S. Work-related stress and intention to leave among midwives working in Swiss maternity hospitals - a cross-sectional study. BMC Health Serv Res. 2021 Jul;21(1):671. DOI: 10.1186/s12913-021-06706-8
[32] Pierce JL, Brown G. Psychological ownership and the physical environment in organizations. In: Ayoko OB, Ashkanasy NM, editors. Organizational Behaviour and the Physical Environment. London: Routledge; 2019. p. 67-95.
[33] Rodríguez-García MC, Martos-López IM, Casas-López G, Márquez-Hernández VV, Aguilera-Manrique G, Gutiérrez-Puertas L. Exploring the relationship between midwives' work environment, women's safety culture, and intent to stay. Women Birth. 2023 Feb;36(1):e10-e16. DOI: 10.1016/j.wombi.2022.04.002
[34] Sander EJ, Caza A, Jordan PJ. The physical work environment and its relationship to stress. In: Ayoko OB, Ashkanasy NM, editors. Organizational Behaviour and the Physical Environment. London: Routledge; 2019. p. 268-84.
[35] Skogström LB, Vithal E, Wijk H, Lindahl G, Berg M. Women's Experiences of Physical Features in a Specially Designed Birthing Room: A Mixed-Methods Study in Sweden. HERD. 2022 Jul;15(3):193-205. DOI: 10.1177/19375867221077097
[36] Stahl K. Arbeitssituation von angestellten Hebammen in deutschen Kreißsälen–Implikationen für die Qualität und Sicherheit der Versorgung [withdrawn]. Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen. 2016. DOI: 10.1016/j.zefq.2016.07.005
[37] Streffing J, Ayerle GM. Konstruktion und Validierung eines Fragebogens zur Arbeitszufriedenheit von Hebammen. In: 6. Internationale Konferenz der Deutschen Gesellschaft für Hebammenwissenschaft; Winterthur. Düsseldorf: German Medical Science GMS Publishing House; 2022.
[38] Sullivan K, Lock L, Homer CS. Factors that contribute to midwives staying in midwifery: a study in one area health service in New South Wales, Australia. Midwifery. 2011 Jun;27(3):331-5. DOI: 10.1016/j.midw.2011.01.007
[39] Symon A, Paul J, Butchart M, Carr V, Dugard P. Maternity unit design study part 2: perceptions of space and layout. Br J Midwifery. 2008;16(2):110-4. DOI: 10.12968/bjom.2008.16.2.28344
[40] Vischer JC. The effects of the physical environment on job performance: towards a theoretical model of workspace stress. Stress and Health. 2007;23(3):175-84. DOI: 10.1002/smi.1134
[41] Wangler S, Simon A, Meyer G, Ayerle GM. Influence of the birthing room design on midwives' job satisfaction - A cross-sectional online survey embedded in the 'Be-Up' study. Sex Reprod Healthc. 2023 Sep;37:100867. DOI: 10.1016/j.srhc.2023.100867
[42] Wangler S, Streffing J, Simon A, Meyer G, Ayerle GM. Measuring job satisfaction of midwives: A scoping review. PLoS One. 2022;17(10):e0275327. DOI: 10.1371/journal.pone.0275327
[43] Warr P, Cook J, Wall T. Scales for the measurement of some work attitudes and aspects of psychological well-being. J Occup Psychol. 1979;52(2):129-48. DOI: 10.1111/j.2044-8325.1979.tb00448.x

