Analysis of Candidozyma auris – an emerging threat in intensive care units
Akshata Uppar 1Saravana Priya Jayakumar Kalpana 1
Veena Kumari Haradara Bahubali 1
1 National Institute of Mental Health and Neurosciences (NIMHANS) Bengaluru, Karnataka, India
Abstract
Introduction: Candidozyma (C.) auris (formerly Candida auris) is an emerging fungus posing a serious global health threat due to its multidrug resistance and difficulty in identification with standard laboratory methods. It causes severe illness in hospitalized patients, with risk factors including recent surgery, diabetes, and the use of broad-spectrum antibiotics and antifungals. Colonization of the respiratory tract, catheters, and skin with C. auris can lead to serious infections, particularly through central venous catheters, urinary catheters, and tracheostomy tubes, resulting in fungemia.
Case series: We present a case series of five ICU patients with fungemia caused by C. auris. The cases emphasize the immune status, screening, and clinical manifestations of these patients. Antifungal susceptibility testing using broth microdilution was performed, and antifungals were administered based on sensitivity reports. Three patients showed improvement with appropriate therapy.
Conclusion: C. auris infections are increasing in prevalence and represent a significant burden to healthcare system and patients. Aggressive treatment and stringent infection control measures are essential to prevent the spread, multi-drug resistance, and mortality associated with C. auris. This study highlights the importance of effective treatment management, including the selection of antifungal agents and the implementation of robust infection control practices, to combat this emerging pathogen.
Keywords
Candidozyma auris, Candida auris, antifungal susceptibility, central venous catheter, colonization, critically ill, emergent pathogen, ICU, infection control, multidrug resistance, nosocomial outbreak
Introduction
Candidozyma (C.) auris (formerly Candida auris), first reported in 2009 in Japan [1], has emerged as a significant nosocomial pathogen. It is associated with outbreaks in intensive care units (ICUs) and poses a major concern despite enhanced infection prevention and control (IPC) measures [2]. Variable antifungal susceptibility and resistance mechanisms further complicate its management [3]. The difficulty in identification using conventional and molecular techniques, coupled with its environmental niches and mechanisms of spread, has hindered the effective control of C. auris infections [4], [5].
The use of prophylactic antifungal agents such as fluconazole has led to an increased prevalence of colonization and infection with non-albicans Candida spp. in recent years [6]. Historically, invasive candidiasis was predominantly caused by Candida albicans [7]. However, with the shift towards non-albicans Candida spp., fluconazole is no longer the mainstay of empirical antifungal treatment [8]. C. auris, with its ability to rapidly spread among critically ill patients, has become a dominant opportunistic pathogen in these individuals [9].
The primary objectives of this study are to investigate the prevalence and characteristics of C. auris infections in ICU settings, evaluate the effectiveness of antifungal treatment, and assess the impact of IPC measures on controlling its spread. By addressing these objectives, the study aims to provide insights into better management practices for this emerging pathogen.
Case description
Case 1
A 36-year-old male was admitted to the emergency department with subdural hematoma and temporal contusion. Following surgery, he was transferred to the ICU due to poor sensorium. A urinary catheter was in place since admission. Upon admission to the ICU, the patient continued to receive mechanical ventilation, and a central line was inserted on the 4th day in the right internal jugular vein. Routine blood investigations, including hemogram, liver, and kidney function tests, were performed. Due to the failure to extubate and worsening chest condition, a CT scan revealed hemopneumothorax, and an implantable cardioverter-defibrillator was placed. The patient improved and was off the ventilator but developed fever. A paired blood culture identified C. auris by MALDI-TOF MS. The central line was removed on the 29th day. The patient was diagnosed with C. auris fungemia and administered caspofungin (loading dose of 70 mg, followed by 50 mg/day). 72 hours after treatment, the patient improved, and a repeated blood culture yielded no growth. The patient was transferred out of the ICU, and discharged with a recommendation to continue caspofungin for 14 days from the last negative blood report. Total ICU days were 44, with 29 days of central line catheter use and 32 days of Foley’s catheter.
Case 2
A 31-year-old male diagnosed with right fronto-temporo-parietal epidural hematoma (EDH) underwent surgery and was shifted to the ICU postoperatively due to failing saturation after EDH surgery. A urinary catheter was in place since admission, and a central line was inserted on the 3rd day in the left internal jugular vein. The patient developed new onset weakness and underwent re-exploration surgery. Suspected pneumonia led to treatment with cefoperazone-sulbactam and amikacin due to endotracheal aspiration yielding Klebsiella spp. The patient was gradually weaned off the ventilator but continued to have fever spikes. Paired blood culture identified C. auris. The central line, in place for 10 days, was suspected of causing a catheter-related bloodstream infection (CRBSI). The patient was treated with caspofungin for 14 days with a loading dose of 70 mg, followed by 50 mg/day. The fever decreased, and repeated blood cultures showed no growth after 48 hours of therapy. The patient was discharged with advice to continue caspofungin for two weeks. Total ICU days were 17, with 10 days of central line catheter use, and 13 days of Foley’s catheter.
Case 3
A 31-year-old male diagnosed with right fronto-temporo-parietal EDH underwent surgery. Postoperatively, the patient experienced dropped saturation and developed bilateral aspiration pneumonitis, leading to ICU admission. A central line was placed on the 3rd day in the left internal jugular vein. Following re-exploration surgery, the patient was weaned off the ventilator and transferred to the normal ward. The patient developed fever, and a workup revealed C. auris in paired blood culture. The central line, in place for 10 days, was suspected of causing CRBSI. Caspofungin was administered for 14 days with loading dose of 70 mg, followed by 50 mg/day), reducing the fever. The patient was discharged, with follow-up blood cultures showing no growth. The patient had no significant medical history and was advised to continue caspofungin for 14 days from the date of the last blood culture showing no growth. Hematological, biochemical, and coagulation profiles were within normal limits. Total device days for the central line were 10, and total ICU days were 44 with 13 days on Foley’s catheter.
Case 4
A 69-year-old male with a left temporal contusion and subarachnoid hemorrhage was admitted to the emergency department and underwent surgery. The patient remained on ventilation, with a urinary catheter and central line placed in the right internal jugular vein on the 3rd day of ICU admission. The patient had continuous fever spikes and elevated total counts. Urine culture identified C. auris with no other positive sites during that period. The patient was not prescribed an antifungal. Blood culture confirmed fungemia after 7 days of incubation. The patient died on day 2 of ICU and day 10 of hospital stay. Total device days for the central line were 10, and total ICU days were 18 with 13 days on a Foley’s catheter.
Case 5
A 67-year-old male diagnosed with multiple central contusions underwent surgery and was admitted to the ICU due to low Glasgow coma scale score. The patient remained on ventilation. Urine culture and subsequent urine culture sensitivity reports identified C. auris with no other positive sites during that period. The patient was not prescribed an antifungal. Blood culture confirmed fungemia after 7 days of incubation. The patient died before the blood culture report showed growth. Total device days for the central line were 12, and total ICU days were 20 with 15 days on a Foley’s catheter.
Cross-sectional data
Identification of C. auris
Identification was performed using MALDI-TOF MS and ensuring accurate species identification.
Antifungal susceptibility testing
Susceptibility to fluconazole, itraconazole, posaconazole, voriconazole, amphotericin B, caspofungin, and anidulafungin was tested using the broth microdilution method.
Patient monitoring
Routine blood investigations, including hemogram, liver and kidney function tests, were conducted. To screen for C. auris, paired blood cultures, urine cultures, and ear swabs are collected using aseptic techniques and promptly transported to the lab. Proper labeling and documentation ensure accurate detection and timely treatment.
Treatment protocol
Caspofungin was started empirically and continued based on sensitivity reports. Patients received a loading dose of 70 mg, followed by 50 mg/day, and adjusted as necessary based on clinical response.
Infection prevention and control (IPC) measures
These included isolation of infected patients, strict hand hygiene, and terminal cleaning of patient rooms with hypochlorite. Environmental screening was conducted to identify potential sources of transmission (Table 1 [Tab. 1]).
Table 1: Infection control measures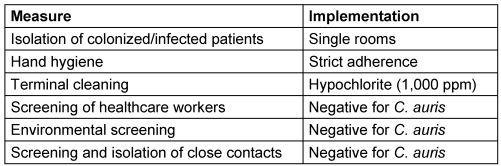
These methods ensure accurate identification, effective treatment, and prevention of C. auris transmission in ICU settings.
Antifungal susceptibility testing
All isolates were tested for susceptibility to fluconazole, itraconazole, posaconazole, voriconazole, amphotericin B, caspofungin, and anidulafungin (Table 2 [Tab. 2]). C. auris was predominantly found in immunocompromised patients, often as a skin or urinary tract colonization. Invasive infections occurred in critically ill patients in ICUs, with major risk factors including recent surgery, diabetes, and broad-spectrum antibiotic use. The mortality rate associated with these infections was above 50% [10].
Table 2: Antifungal susceptibility testing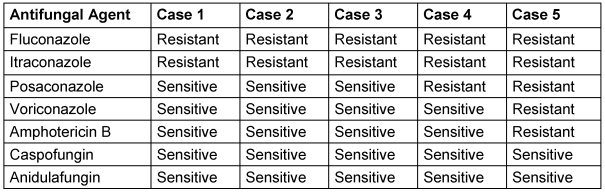
Summary of the case series
Out of 5 patients with C. auris infections (fungemia and CRBSI), 3 were treated with caspofungin and recovered, 2 patients who did not receive antifungal treatment expired (Table 3 [Tab. 3]).
Table 3: Comprehensive analysis of C. auris infections: clinical manifestations, therapeutic interventions, and hospitalization metrics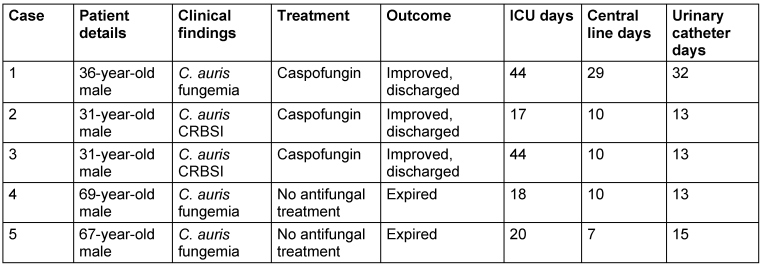
Discussion
This study presents a cluster of cases with probable acquisition of infection by case 1 from the environment of the critical care unit, and subsequent colonization and infection of the other patients in the following months. Out of 5 patients, 3 were treated with antifungals and recovered, 2 patients who did not receive antifungal treatment expired.
C. auris is found mainly in immunocompromised patients in ICUs as a skin or urinary tract colonization. Invasive infection occurs in critically ill patients in intensive care units with major risk factors and are associated with a mortality rate above 50% [11], [12], [13], [14].
C. auris is capable of surviving on surfaces for extended periods. After seven days, approximately 38% of the yeast remains cultivable on dry surfaces, while about 93% persists on moist surfaces. On stainless steel with an initial inoculum of ~4.8 lg colony-forming units (cfu), approximately ~3.5 lg cfu remain after 4 days and ~0.4 lg cfu after 14 days. On plastic surfaces, biofilm formation with an initial inoculum of ~8 lg cfu results in ~4.3 lg cfu being recultivable after 14 days.
This highlights the importance of thorough and frequent cleaning in healthcare settings. Effective disinfection practices, using disinfectants proven effective against C. auris, are essential for preventing the spread of this resilient pathogen in such environments [15], [16].
Routine screening and surveillance are vital for early detection of C. auris colonization and infection. Protocols for screening healthcare workers and patients, especially in high-risk areas such as ICUs, should be implemented. Effective screening helps identify and isolate colonized patients, preventing further transmission [17]. Environmental sampling and screening of healthcare workers (HCWs) and all close contacts (patients in the same ICU) was carried out; the screening results were negative [18].
Patients colonized or infected with C. auris should be isolated in single rooms with dedicated bathroom facilities. Isolation helps contain the spread of the pathogen within healthcare settings. Managing isolated patients requires meticulous planning and adherence to infection control protocols [19].
The following measures were implemented: standard precautions including hand hygiene were strictly adhered to and all infected patients with C. auris were isolated in a single room, with the room terminally cleaned after discharge using a hypochlorite solution at 1,000 ppm of available chlorine (i.e., a concentration higher than that routinely used).
Hand hygiene is a cornerstone of infection control. HCWs adhered to strict hand hygiene protocols, including the use of alcohol-based hand rubs and regular hand washing. The importance of proper hand hygiene and the use of personal protective equipment cannot be overstated in preventing the transmission of C. auris [20].
All isolates were subjected to antifungal susceptibility testing against fluconazole, itraconazole, posaconazole, voriconazole, amphotericin B, caspofungin, and anidulafungin [21], [22].
Treating C. auris infections is challenging due to the increasing reports of echinocandin-resistant and pan-resistant strains. In this study, three out of five patients were treated with antifungals and recovered, while the two who did not receive antifungal treatment died. Early detection and appropriate antifungal therapy are essential for improving patient outcomes [23].
Managing C. auris clusters/outbreaks requires a coordinated approach, including contact tracing, patient transfers, and additional screening measures. Public health departments play a crucial role in monitoring outbreaks and implementing control measures. Reporting cases to state or local health authorities is necessary for effective outbreak management [24].
Patients often remain colonized with C. auris for long periods, even after treatment. Long-term infection control measures, including regular monitoring of colonized patients, are necessary to prevent recurrence and further spread [24].
Educating HCWs about C. auris, its transmission, and infection control measures is essential. Regular training sessions and updates on the latest guidelines and recommendations help ensure that HCWs are equipped to manage C. auris infections effectively [25], [26].
Conclusion
C. auris infections are increasing in prevalence and represent a significant burden to the healthcare system and patients. An aggressive approach to treating C. auris in most patients is essential to prevent subsequent invasive spread, multi-drug resistance, and ultimately, mortality. To achieve this, it is imperative that detailed information regarding C. auris urinary and blood isolation, concomitantly positive sites, treatment management – including both infection control measures and antifungal agent selection – and duration of therapy, be collected and disseminated. This will enable the design of effective, evidence-based treatment regimens for patients infected with C. auris. Moving forward, a coordinated effort is required to address the challenges posed by C. auris and to implement effective strategies to manage and control its spread.
Notes
Authors’ ORCIDs
- Saravana Priya Jayakumar Kalpana: https://orcid.org/0000-0002-1143-8206
Ethical approval
The project was approved by the Institutional Ethics Committee and all patients gave written consent before participation after adequate explanation. Informed consent from patients was obtained, and careful measures were taken to maintain confidentiality regarding the identity of these patients.
Funding
None.
Competing interests
The authors declare that they have no competing interests.
References
[1] Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009 Jan;53(1):41-4. DOI: 10.1111/j.1348-0421.2008.00083.x[2] Cortegiani A, Misseri G, Giarratano A, Bassetti M, Eyre D. The global challenge of Candida auris in the intensive care unit. Crit Care. 2019 May;23(1):150. DOI: 10.1186/s13054-019-2449-y
[3] Chaabane F, Graf A, Jequier L, Coste AT. Review on Antifungal Resistance Mechanisms in the Emerging Pathogen Candida auris. Front Microbiol. 2019;10:2788. DOI: 10.3389/fmicb.2019.02788
[4] Du H, Bing J, Hu T, Ennis CL, Nobile CJ, Huang G. Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020 Oct;16(10):e1008921. DOI: 10.1371/journal.ppat.1008921
[5] Keighley C, Garnham K, Harch SAJ, Robertson M, Chaw K, Teng JC, Chen SC. Candida auris: Diagnostic Challenges and Emerging Opportunities for the Clinical Microbiology Laboratory. Curr Fungal Infect Rep. 2021;15(3):116-26. DOI: 10.1007/s12281-021-00420-y
[6] Ganguli SC, Edirisinghe VT, Dasanayaka PN, Wijendra WAS. Review of Candida auris - An emerging global threat. Curr Res Environ Appl Mycol. 2024;14(1):133-45. DOI: 10.5943/cream/14/1/8
[7] Giacobbe DR, Mikulska M, Vena A, Di Pilato V, Magnasco L, Marchese A, Bassetti M. Challenges in the diagnosis and treatment of candidemia due to multidrug-resistant Candida auris. Front Fungal Biol. 2023;4:1061150. DOI: 10.3389/ffunb.2023.1061150
[8] Lee Y, Robbins N, Cowen LE. Molecular mechanisms governing antifungal drug resistance. NPJ Antimicrob Resist. 2023;1(1):5. DOI: 10.1038/s44259-023-00007-2
[9] Barbian HJ, Lie L, Kittner A, Harrington A, Carson J, Frias M, Slade DH, Kim DY, Black S, Parada JP, Hayden MK. Candida auris Outbreak and Epidemiologic Response in Burn Intensive Care Unit, Illinois, USA, 2021-2023. Emerg Infect Dis. 2025 Mar;31(3):438-47. DOI: 10.3201/eid3103.241195
[10] Nandini D, Manonmoney J, Lavanya J, Leela KV, Sujith. A Study on prevalence and characterization of candida species in immunocompromised patients. J Pure Appl Microbiol. 2023;17(1):427-33. DOI: 10.22207/JPAM.15.4.29
[11] McDougal AN, DeMaet MA, Garcia B, York T, Iverson T, Ojo O, Patel J. A cluster investigation of Candida auris among hospitalized incarcerated patients. Antimicrob Steward Healthc Epidemiol. 2023;3(1):e244. DOI: 10.1017/ash.2023.520
[12] Sathyapalan DT, Antony R, Nampoothiri V, Kumar A, Shashindran N, James J, Thomas J, Prasanna P, Sudhir AS, Philip JM, Edathadathil F, Prabhu B, Singh S, Moni M. Evaluating the measures taken to contain a Candida auris outbreak in a tertiary care hospital in South India: an outbreak investigational study. BMC Infect Dis. 2021 May;21(1):425. DOI: 10.1186/s12879-021-06131-6
[13] Koleri J, Petkar HM, Rahman S Al Soub HA, Rahman S AlMaslamani MA. Candida auris Blood stream infection - a descriptive study from Qatar. BMC Infect Dis. 2023 Aug;23(1):513. DOI: 10.1186/s12879-023-08477-5
[14] Geremia N, Brugnaro P, Solinas M, Scarparo C, Panese S. Candida auris as an Emergent Public Health Problem: A Current Update on European Outbreaks and Cases. Healthcare (Basel). 2023 Feb;11(3):425. DOI: 10.3390/healthcare11030425
[15] Kramer A, Lexow F, Bludau A, Köster AM, Misailovski M, Seifert U, Eggers M, Rutala W, Dancer SJ, Scheithauer S. How long do bacteria, fungi, protozoa, and viruses retain their replication capacity on inanimate surfaces? A systematic review examining environmental resilience versus healthcare-associated infection risk by "fomite-borne risk assessment". Clin Microbiol Rev. 2024 Dec;37(4):e0018623. DOI: 10.1128/cmr.00186-23
[16] Welsh RM, Bentz ML, Shams A, Houston H, Lyons A, Rose LJ, Litvintseva AP. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J Clin Microbiol. 2017 Oct;55(10):2996-3005. DOI: 10.1128/JCM.00921-17
[17] Banik S, Ozay B, Trejo M, Zhu Y, Kanna C, Santellan C, Shaw B, Chandrasekaran S, Chaturvedi S, Vejar L, Chakravorty S, Alland D, Banada P. A simple and sensitive test for Candida auris colonization, surveillance, and infection control suitable for near patient use. J Clin Microbiol. 2024 Jul;62(7):e0052524. DOI: 10.1128/jcm.00525-24
[18] Chowdhary A, Sharma C, Meis JF. Candida auris: A rapidly emerging cause of hospital-acquired multidrug-resistant fungal infections globally. PLoS Pathog. 2017 May;13(5):e1006290. DOI: 10.1371/journal.ppat.1006290
[19] Yadav A, Singh A, Wang Y, Haren MHV, Singh A, de Groot T, Meis JF, Xu J, Chowdhary A. Colonisation and Transmission Dynamics of Candida auris among Chronic Respiratory Diseases Patients Hospitalised in a Chest Hospital, Delhi, India: A Comparative Analysis of Whole Genome Sequencing and Microsatellite Typing. J Fungi (Basel). 2021 Jan;7(2):81. DOI: 10.3390/jof7020081
[20] Ahmad S, Asadzadeh M. Strategies to Prevent Transmission of Candida auris in Healthcare Settings. Curr Fungal Infect Rep. 2023;17(1):36-48. DOI: 10.1007/s12281-023-00451-7
[21] Jeffery-Smith A, Taori SK, Schelenz S, Jeffery K, Johnson EM, Borman A; Candida auris Incident Management TeamManuel R, Brown CS. Candida auris: a Review of the Literature. Clin Microbiol Rev. 2018 Jan;31(1):e00029-17. DOI: 10.1128/CMR.00029-17
[22] Siopi M, Pachoulis I, Leventaki S, Spruijtenburg B, Meis JF, Pournaras S, Vrioni G, Tsakris A, Meletiadis J. Evaluation of the Vitek 2 system for antifungal susceptibility testing of Candida auris using a representative international panel of clinical isolates: overestimation of amphotericin B resistance and underestimation of fluconazole resistance. J Clin Microbiol. 2024 Apr;62(4):e0152823. DOI: 10.1128/jcm.01528-23
[23] Jacobs SE, Jacobs JL, Dennis EK, Taimur S, Rana M, Patel D, Gitman M, Patel G, Schaefer S, Iyer K, Moon J, Adams V, Lerner P, Walsh TJ, Zhu Y, Anower MR, Vaidya MM, Chaturvedi S, Chaturvedi V. Candida auris Pan-Drug-Resistant to Four Classes of Antifungal Agents. Antimicrob Agents Chemother. 2022 Jul;66(7):e0005322. DOI: 10.1128/aac.00053-22
[24] Hayes JF. Candida auris: Epidemiology Update and a Review of Strategies to Prevent Spread. J Clin Med. 2024 Nov;13(22):6675. DOI: 10.3390/jcm13226675
[25] Centers for Disease Control and Prevention. Infection control guidance: Candida auris. 2024 Apr 24. Available from: https://www.cdc.gov/candida-auris/hcp/infection-control/index.html.
[26] Carty J, Chowdhary A, Bernstein D, Thangamani S. Tools and techniques to identify, study, and control Candida auris. PLoS Pathog. 2023 Oct;19(10):e1011698. DOI: 10.1371/journal.ppat.1011698

