Fungal spinal infections: a narrative review on diagnosis, treatment strategies, and collaborative management approaches
Anand Kumar Das 1Mainak Sinha 2
Rijhul Lahariya 3
Saraj Kumar Singh 1
Sona Bhardwaj 4
Simmi Kishore 5
1 MCh Neurosurgery, All India Institute of Medical Sciences, Patna, Bihar, India
2 Department of General Surgery, All India Institute of Medical Sciences, Patna, Bihar, India
3 MBBS, All India Institute of Medical Sciences, Patna, Bihar, India
4 Department of Microbiology, ESIC Hospital, Patna, Bihar, India
5 Department of Anaesthesiology and Critical Care Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India
Abstract
Introduction: Spinal fungal infections are rare with a frequency of 2.2 times per 100,000 people annually. They are caused by pathogens such Coccidioides immitis, Blastomyces dermatitidis, Cryptococcus neoformans, Candida albicans, and Aspergillus fumigatus (found globally).
This review on fungal spinal infections examines patient demographics, medicinal treatments, surgical methods, and outcomes.
Method: All PubMed articles on fungal spine infections were analysed, regardless of fungus, publication year, or spinal segment. The patient’s age, gender, affected spinal section, microorganism, treatment regimens, surgical methods, follow-up period, and results were recorded.
Results: Of the 134 analyzed patients, 66.4% were male. The mean age was 54.3±14.9 years. Most susceptible was the lumbar spine (47%), followed by the thoracic (29.9%) and lumbo-sacral (12.7%). The most common organism was Candida albicans (62.7%), followed by Aspergillus fumigatus (27.6%). Spondylodiscitis (35.8%) and osteomyelitis (31.3%) lead our review.
The most frequent antifungals were triazoles (55%), followed by polyenes (31%). Most procedures (59.5%) were non-fixation.
Back discomfort, fever, and neurological impairments were prominent signs of spine fungal infections. Blood tests, cultures, and MRI/CT scans were used to diagnose.
Spondylodiscitis had a letality of 6.25%, spinal osteomyelitis of 11%. Recovery requires long-term monitoring.
Conclusion: The review emphasises the significance of early detection and treatment, individualised antifungal regimens, and surgery in specific cases to enhance fungal spinal infection outcomes. Spine surgeons and radiologists must work together to solve diagnostic and therapeutic issues.
Keywords
fungal infections, spine infections, vertebral osteomyelitis, spondylodiscitis, anti-fungal drugs
Introduction
Fungal infections of the spine are relatively uncommon. The complexity of diagnosing and treating spinal infections often demands a collaborative, cross-disciplinary approach involving spine surgeons and radiologists. The primary causes of spinal infections tend to be bacterial or fungal pathogens entering through the bloodstream, with Staphylococcus aureus and Escherichia coli being the most prevalent bacteria responsible for such infections [1].
Specific fungi like Coccidioides immitis and Blastomyces dermatitidis limited to certain geographical areas, while others like Cryptococcus spp., Candida spp., and Aspergillus spp. are found worldwide [2]. Coccidioidomycosis and Blastomycosis is prevalent in the American region [2]. Aspergillosis and Mucormycosis is more prevalent in the Asian region, especially in India [3].
The incidence rate of spinal infections is roughly 2.2 new cases annually per 100,000 individuals [4]. Spinal infections can be grouped according to the precise anatomical location impacted, including the vertebrae, intervertebral discs, spinal canal, and adjacent soft tissues [1]. The lumbar region is the area of the spine most commonly involved in spinal infections, followed by the thoracic and cervical regions, while hematogenous spread of infection to the sacral spine is relatively rare [4].
This is a comprehensive review of spinal infections caused by various fungi, presented according to the region in the spine affected, with patient’s demographic details, their medical therapy and surgical management, and follow-up along with their eventual outcome. This study explored studies from various parts of the world and is presented in this review article.
Method
This review article has included articles published in National Library of Medicine (PubMed), using the search syntax ([mycotic OR fungal OR infection OR candida OR spondylodiscitis OR osteomyelitis] AND [spine OR spinal]). We included all fungal infections related to any segment of the spine. We tried to collect all relevant data from each of the articles including, age and gender of the patient, their spinal segment, the fungus involved, their follow-up duration, their medical therapy and surgical intervention, the main diagnosis of the patient and the overall outcome of the patient.
We included all patient above the age of 18 years, and made no restrictions on gender. We also made no restrictions related to any fungus, year of publication, follow-up duration or spinal segment. Articles in English literature only, from all over the world were included in this review. In medical therapy, we collected the details about the antifungal drug regimen used for the patient with the class of drug used. Under surgical intervention, we gathered the details about whether any intervention done or not. If yes, then was it without fixation or with fixation. Outcomes parameters included the follow-up duration of the patient, and their recovery and mortality status. Tab. 1 in the supplement (Attachment 1 [Att. 1]) shows all studies included in this review.
Results
The mean age of the included patients was 54.3 years±14.9 years. 89 were male (66.4%). The distribution of affected spinal regions varied, with the most common being lumbar (47%), followed by thoracic (29.9%), and lumbo-sacral (12.7%). Candida spp. were the most prevalent organisms identified, accounting for 62.7% of cases, followed by Aspergillus spp. (27.6%), with other organisms being relatively rare. Spondylodiscitis was the most frequent diagnosis (35.8%), followed by osteomyelitis (31.3%), and discitis (17.9%). Triazoles were most prescribed in 55% of cases, followed by polyenes (31%), and echinocandins (8.5%). The majority of interventions involved surgery, with 59.5% undergoing surgery without fixation and 40.5% undergoing surgery with fixation. Among these, the most common cause of surgery with fixation was discitis. Among the 131 individuals with reported outcomes, 90.1% were alive at the conclusion of the study, while 9.9% had died. The most common cause of death among the participants was spinal abscess (38.5%). The mean follow-up period (in months) for participants included in this review was 18.5 months±15 months (Table 1 [Tab. 1]).
Table 1: Demographics of the patient population, affected spine region, isolated fungi and therapy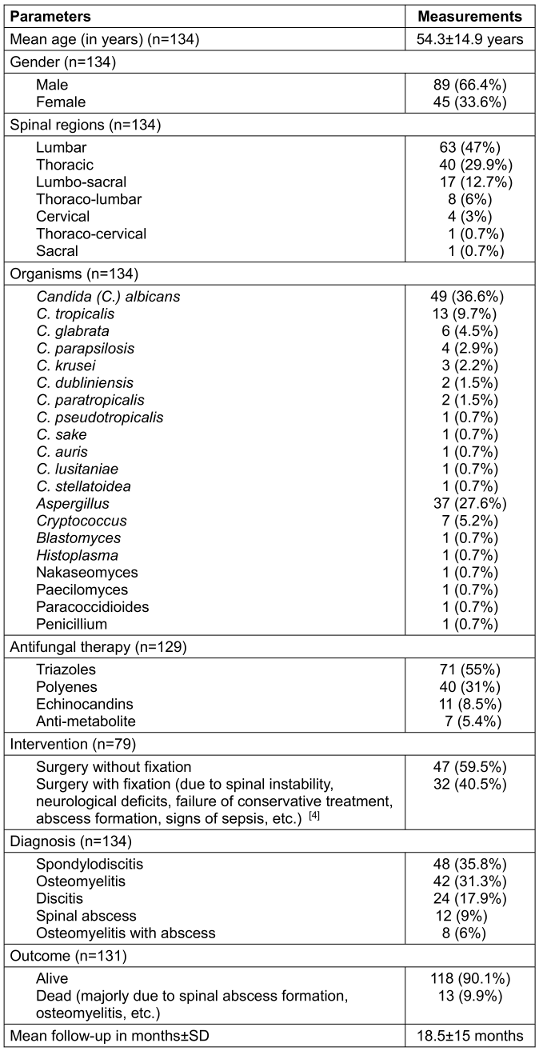
The fungal detection in various spine regions is summarised in Table 2 [Tab. 2]. Only Aspergillus, Candida and Cryptococcus spp. were detected in different regions.
Table 2: Distribution of different fungi within the spine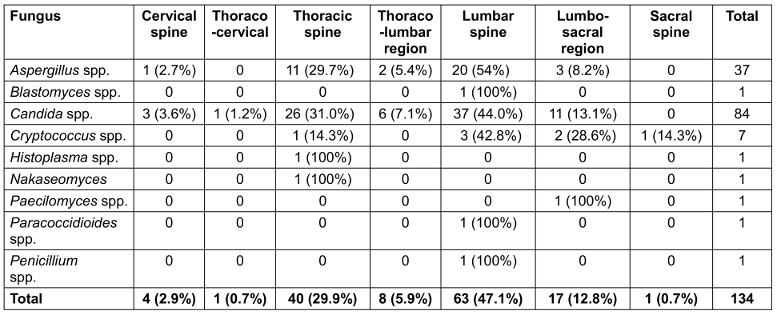
Table 3 [Tab. 3] is the summarised form of all the details about the participants we included, according to the diseases.
Table 3: Detailed review of all articles on the basis of the diagnosis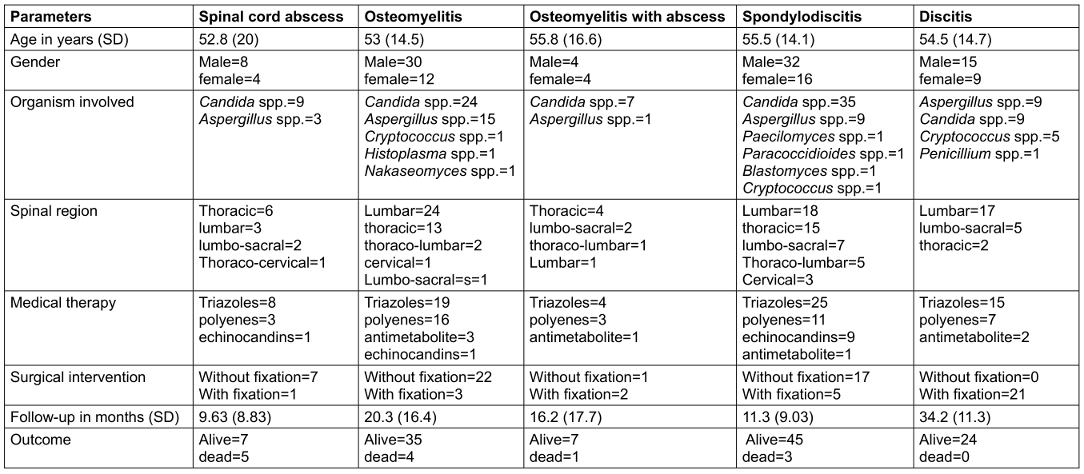
Discussion
Etiology
Candida and Aspergillus spp. are the most common causes of fungal vertebral osteomyelitis in immunocompromised patients [5]. Candida spp. were the most prevalent fungi, followed by Aspergillus, Cryptococcus, Histoplasma and Nakaseomyces spp. Candida and Aspergillus spp. were also the most common microorganisms for causing spinal cord abscess, a complication of osteomyelitis, caused most commonly by Candida spp. This finding was supported by other articles too [6], [7]. The most common microorganisms causing spondylodiscitis were found to be Candida and Aspergillus spp. in the reviewed articles. In rare cases Blastomyces, Paracoccidioides, Cryptococcus and Paecilomyces spp. causing spondylodiscitis. Among the discitis patients, the most common organisms involved were Candida and Aspergillus spp., few cases of Cryptococcus spp. and there was one case of Penicillium spp. infection. This was also supported by a few more studies [8], [9], [10].
Presentation
From the articles reviewed, the mean age of vertebral osteomyelitis presentation was 53 years with a standard deviation of 14.5 years, with a male predominance, which corresponds with other studies [1], [11]. The most prevalent site affected was the lumbar spine, followed by the thoracic spine and the thoraco-lumbar region, supporting the current evidence [12]. The common symptoms that patients present with are back pain, fever, chills, muscle spasms, weight loss, and neurological deficits like numbness and weakness, like reported in the literature [1]. Spinal cord abscess is more prevalent in the population of males over 52.8 years with a standard deviation of 20 years [1], [13]. Thoracic spine was the most frequently affected, followed by the lumbar and lumbo-sacral regions. The common symptoms that patients present with spinal abscess include fever, chills, loss of bladder and bowel control, loss of sensation in the body area below the abscess, headache, and muscle weakness, especially in the legs [6], [14], [15]. In spondylodiscitis, males are affected more, in the age group of 55.5 years with a standard deviation of 14.1 years, analogous as reported of Yu et al. [16]. In accordance with the literature [16], [17], the most common site affected by spondylodiscitis was the lumbar spine, followed by the thoracic spine and the lumbo-sacral region. The most common manifestation was lower back pain, with other features like fever, chills, some neurological manifestations, an abscess, and sometimes vertebral collapse, which corresponds with the literature [17], [18], [19]. Discitis has a higher incidence among the 50-year-old age group, with male predominance as also reported in the literature [10].
The mean age of the patients who had discitis was 54.5 years (SD 14.7 years) with male percentage of 62.5%.
The lumbar region was to be most affected, followed by the lumbo-sacral and thoracic regions, which corresponds with the literature [9]. In accordance to the literature [20], [21], [22], the common signs and symptoms of discitis include non-relieving back pain or neck pain, fever, weight loss, motor weakness that eventually causes paralysis, abdominal discomfort, and sensory impairment.
Diagnosis
The diagnosis of vertebral osteomyelitis is somewhat dependent on several blood tests and imaging techniques. Complete blood count, erythrocyte sedimentation rate, and C-reactive protein are reliable indicators of inflammation [1], [23]. Blood culture is done to find out the organism involved along with its species for effective antibiotic treatment and intervention [23]. Imaging tools are available that are effective in making a diagnosis. A computed tomography (CT) scan is best to diagnose the structural deformity of the bone. Magnetic Resonance Imaging (MRI) is considered the gold standard as it can view infected tissues like muscles, nerves involved, and other soft tissues [1]. Gallium-67 single-photon emission computed tomography (SPECT) was being used as an alternative to MRI with sensitivity comparable to MRI in patients where MRI was contraindicated [23], [24]. And if the doubt persists, a biopsy is done using CT-guided aspiration or biopsy. MRI is also helpful in guiding the site for CT-guided tissue biopsy [23].
The diagnosis of spinal cord abscess is generally made by considering inflammatory markers like white blood cell count (WBC), erythrocyte sedimentation rate (ESR), and c-reactive protein (CRP), which will be raised [6], [13], [15]. Culture can be done with the pus and/or blood sample to find the causative organism for effective treatment. Among various imaging techniques, MRI with gadolinium is the most reliable technique to detect spinal abscesses with sensitivity and specificity above 90% [13], [15]. It also aids in the detection of vertebral osteomyelitis, which is the primary risk factor for spinal cord abscess. Other techniques, like CT with intravenous contrast media, are considered an alternative choice for diagnosis [6], [13], [15].
The mainstay of the treatment remains antibiotic therapy, but the surgeon needs to drain the abscess with a needle to release the pressure [15]. Other procedures, like laminectomy and corpectomy, can be employed to drain the abscess [6]. In many of the cases, the culture may give a false negative result, so early CT-guided needle aspiration of the abscess is to be done [13].
The diagnosis of spondylodiscitis depends on laboratory and imaging techniques. Routine inflammation markers, including ESR and CRP, are usually a bit elevated. MRI stands out as the most sensitive imaging technique for making the diagnosis. Thorough investigations related to the microbiological tests should be done to confirm the infective organisms for effective antifungal therapy. A CT-guided biopsy and fine needle aspiration cytology are done to confirm the diagnosis and for proper management of the condition [16], [19]. Delayed diagnosis and initiation of antifungals would lead to a poor outcome [19].
The first step in diagnosing discitis is to check for the infection through inflammatory markers like ESR and CRP that are likely to be raised [21]. A positive blood culture is needed to find the causative organism, whether it’s fungal, bacterial, or parasitic, to start the correct antibiotic regime [21]. MRI is considered to be the most sensitive and better diagnostic technique, but the gold standard approach is the CT-guided tissue biopsy [10], [21].
Management
The mainstay treatment for vertebral osteomyelitis is the antifungal therapy, along with the immobilisation for increased time in the patient with severe back pain and spinal deformity, followed by rehabilitation exercises for muscle strengthening [1], [23]. In our review, the most commonly used antifungal was triazoles like voriconazole, fluconazole, and itraconazole, followed by polyenes like nystatin, amphotericin B, liposomal preparation of amphotericin B and few cases with antimetabolite group of drugs. Non-surgical intervention is considered primarily if no severe complications present or no severe symptoms develop in the patient, like a neurological deficit [1]. Surgical intervention has higher mortality rates and includes either debridement of the tissue that is infected or the use of instrumentation to fix the spine to gain stability [1]. Still, many of the patients have poor quality of life as the recovery is prolonged [23]. In our review, the majority of the cases were managed with some intervention without any fixation and just debridement of the infected tissue, with a single case of management with fixation of the spine.
For spinal cord abscess treatment, azoles and polyene groups of drugs were the mainstays of antifungal therapy. The majority of the cases reported were managed with surgical intervention but without any fixation; just laminectomy, corpectomy, and decompression for drainage of the abscess were the primary procedures.
Among the antifungals for the treatment of spondylodiscitis, amphotericin B and azoles are considered the primary antifungal therapies. In our review, azole were used in the majority of the cases, followed by polyenes and echinocandine, which were equally used. If neurological symptoms persist or vertebral collapse is present, only then are surgical interventions considered [19]. Around 80% of the cases were managed with slight intervention but without any fixation. Early decompression enhances the functional recovery of most patients. Just debridement and draining the abscess treat the patient, along with stabilising the spine, as summarized by Caldera et al. [19].
The main antifungal therapies advised to the patient in our review were triazoles and polyenes, including voriconazole, fluconazole, itraconazole and amphotericin B respectively. Surgical intervention is indicated only when some neurological deficits are observed, such as abscess formation that needs to be drained, vertebral cord prolapse, or chronic illness. Decompression for drainage of the abscess was done, and surgical debridement was done for effective medical therapy. In our review, all cases reported for discitis were managed with surgical intervention with fixation of the spinal cord. After fixation, timely follow-up is very much required.
Prognosis
In case of vertebral osteomyelitis, timely follow-up is very necessary for the patient to make a functional recovery as soon as possible. The mean follow-up time for the patient was 20.3 months (SD 16.4 months). And because of that, the mortality rate among the articles we reviewed for vertebral osteomyelitis was around 11%. The common causes of death among patients of osteomyelitis were progression to sepsis, which is a life threatening condition. Patients with compromised immune systems were also at great risk [4]. Among the spinal cord abscess patients, more than half of the cases were reported as alive, with a mean follow-up time of 9.63 months (SD 8.83 months). In case of spondylodiscitis, the mean follow-up time was found to be 11.3 months (SD 9.03 months). And because the majority of the patients were managed with minor procedures and without any fixation, the mortality rate was found to be only 6.25% in patients with spondylodiscitis. Short-term mortality is associated with severe neurologic deficits, epidural abscess, and comorbidities. Long term mortality is related to alcohol dependency [25]. Among the discitis patients, the mean time of follow-up was 34.2 months (SD 11.3 months). After fixing the cord, there was zero mortality rate among the patients reported in our review.
Conclusion
Fungal infections involving the spinal column, comprises of vertebral osteomyelitis, spinal cord abscess formation, spondylodiscitis, and discitis, present significant diagnostic hinderance that are frequently overlooked due to their infrequent occurrence and nonspecific symptoms. Timely diagnosis necessitates a synergistic approach, combining laboratory analysis and advanced imaging techniques, with MRI emerging as the diagnostic gold standard. Effective management of these conditions requires a multidisciplinary treatment strategy, integrating antifungal pharmacotherapy and surgical interventions when deemed appropriate. Despite the intricacies associated with the management of these conditions, timely intervention and a comprehensive care approach contribute to favorable clinical outcomes, underscoring the paramount importance of heightened clinical vigilance and collaborative interdisciplinary practice in addressing these rare yet consequential pathologies.
Notes
Authors’ ORCIDs
- Das AK: 0000-0002-0705-9393
- Sinha M: 0000-0002-2286-0701
- Lahariya R: 0009-0003-5769-4509
- Singh SK: 0000-0003-3156-7096
Contribution
Authors Anand Kumar Das and Mainak Sinha contributed equally.
Funding
None.
Acknowledgments
The authors acknowledge all professors and consultants in the department of Neurosurgery for their guidance and assistance.
Competing interests
The authors declare that they have no competing interests.
References
[1] Spinal Infection – Causes, Symptoms and Treatments. [cited 2024 Feb 21]. Available from: https://www.aans.org/[2] Kim CW, Perry A, Currier B, Yaszemski M, Garfin SR. Fungal infections of the spine. Clin Orthop Relat Res. 2006 Mar;444:92-9. DOI: 10.1097/01.blo.0000203451.36522.4c
[3] Slavin MA, Chakrabarti A. Opportunistic fungal infections in the Asia-Pacific region. Med Mycol. 2012 Jan;50(1):18-25. DOI: 10.3109/13693786.2011.602989
[4] Tsantes AG, Papadopoulos DV, Vrioni G, Sioutis S, Sapkas G, Benzakour A, Benzakour T, Angelini A, Ruggieri P, Mavrogenis AF, World Association Against Infection In Orthopedics And Trauma W A I O T Study Group On Bone And Joint Infection Definitions. Spinal Infections: An Update. Microorganisms. 2020 Mar 27;8(4):476. DOI: 10.3390/microorganisms8040476
[5] Tokuyama T, Nishizawa S, Yokota N, Ohta S, Yokoyama T, Namba H. Surgical strategy for spondylodiscitis due to Candida albicans in an immunocompromised host. Neurol Med Chir (Tokyo). 2002 Jul;42(7):314-7. DOI: 10.2176/nmc.42.314
[6] Raj KA, Srinivasamurthy BC, Nagarajan K, Sinduja MG. A rare case of spontaneous Aspergillus spondylodiscitis with epidural abscess in a 45-year-old immunocompetent female. J Craniovertebr Junction Spine. 2013 Jul;4(2):82-4. DOI: 10.4103/0974-8237.128538
[7] Saigal G, Donovan Post MJ, Kozic D. Thoracic intradural Aspergillus abscess formation following epidural steroid injection. AJNR Am J Neuroradiol. 2004 Apr;25(4):642-4.
[8] Palmisano A, Benecchi M, De Filippo M, Maggiore U, Buzio C, Vaglio A. Candida sake as the causative agent of spondylodiscitis in a hemodialysis patient. Spine J. 2011 Mar;11(3):e12-6. DOI: 10.1016/j.spinee.2011.01.026
[9] Chen H, Lin E. MRI images of a patient with spondylodiscitis and epidural abscess after stem cell injections to the spine. Int J Case Rep Images. 2012 Apr 27;3(8):62-4. DOI: 10.5348/ijcri-2012-08-170-CI-17
[10] Aurora Health Care. Discitis Osteomyelitis. [cited 2024 Mar 24]. Available from: https://www.aurorahealthcare.org/services/aurora-spine-services/spinal-infections/discitis-osteomyelitis
[11] Graeber A, Cecava ND. Vertebral Osteomyelitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Mar 23]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK532256/
[12] Oksi J, Finnilä T, Hohenthal U, Rantakokko-Jalava K. Candida dubliniensis spondylodiscitis in an immunocompetent patient. Case report and review of the literature. Med Mycol Case Rep. 2014 Jan;3:4-7. DOI: 10.1016/j.mmcr.2013.11.001
[13] Sendi P, Bregenzer T, Zimmerli W. Spinal epidural abscess in clinical practice. QJM. 2008 Jan;101(1):1-12. DOI: 10.1093/qjmed/hcm100
[14] MedlinePlus Medical Encyclopedia. Spinal cord abscess. [cited 2024 Mar 24]. Available from: https://medlineplus.gov/ency/article/001405.htm
[15] Columbia Neurosurgery in New York City [Internet]. Epidural Abscess Diagnosis & Treatment - NYC. 2021 [cited 2024 Mar 24]. Available from: https://www.neurosurgery.columbia.edu/patient-care/conditions/epidural-abscess
[16] Yu LD, Feng ZY, Wang XW, Ling ZH, Lin XJ. Fungal spondylodiscitis in a patient recovered from H7N9 virus infection: a case study and a literature review of the differences between Candida and Aspergillus spondylodiscitis. J Zhejiang Univ Sci B. 2016 Nov.;17(11):874-81. DOI: 10.1631/jzus.B1600077
[17] Keerthi C I, Bhat S, Mulki SS, Bhat K A. Fungal infections of spine: Case series during the COVID times. Indian J Med Microbiol. 2022;40(4):605-7. DOI: 10.1016/j.ijmmb.2022.07.002
[18] Iwata A, Ito M, Abumi K, Sudo H, Kotani Y, Shono Y, Minami A. Fungal spinal infection treated with percutaneous posterolateral endoscopic surgery. J Neurol Surg A Cent Eur Neurosurg. 2014 May;75(3):170-6. DOI: 10.1055/s-0032-1329268
[19] Caldera G, Cahueque Lemus MA. Fungal Spondylodiscitis: Review. J Spine. 2016;05(02). [cited 2024 Mar 24]. Available from: http://www.omicsgroup.org/journals/fungal-spondylodiscitis-review-2165-7939-1000302.php?aid=72434
[20] Vertebral osteomyelitis and discitis in adults. UpToDate. [cited 2024 Mar 24]. Available from: https://uptodatefree.ir/topic.htm?path=vertebral-osteomyelitis-and-discitis-in-adults
[21] Advanced Orthopaedics & Sports Medicine, Orthopaedic Specialists, Cypress, Houston, TX. Discitis. [cited 2024 Mar 24]. Available from: https://www.advancedosm.com/discitis-orthopaedic-sports-medicine-specialist-cypress-houston-tx/
[22] Douraiswami B, Subramani S, Varman M. Unprecedented clinical presentation of fungal spondylodiscitis as an extradural mass in an immunocompetent individual. J Clin Orthop Trauma. 2020;11(5):942-6. DOI: 10.1016/j.jcot.2019.08.002
[23] Grammatico L, Baron S, Rusch E, Lepage B, Surer N, Desenclos JC, Besnier JM. Epidemiology of vertebral osteomyelitis (VO) in France: analysis of hospital-discharge data 2002-2003. Epidemiol Infect. 2008 May;136(5):653-60. DOI: 10.1017/S0950268807008850
[24] Love C, Patel M, Lonner BS, Tomas MB, Palestro CJ. Diagnosing spinal osteomyelitis: a comparison of bone and Ga-67 scintigraphy and magnetic resonance imaging. Clin Nucl Med. 2000 Dec;25(12):963-77. DOI: 10.1097/00003072-200012000-00002
[25] Kehrer M, Pedersen C, Jensen TG, Hallas J, Lassen AT. Increased short- and long-term mortality among patients with infectious spondylodiscitis compared with a reference population. Spine J. 2015 Jun;15(6):1233-40. DOI: 10.1016/j.spinee.2015.02.021
[26] Son JM, Jee WH, Jung CK, Kim SI, Ha KY. Aspergillus spondylitis involving the cervico-thoraco-lumbar spine in an immunocompromised patient: a case report. Korean J Radiol. 2007;8(5):448-51. DOI: 10.3348/kjr.2007.8.5.448
[27] D'Agostino C, Scorzolini L, Massetti AP, Carnevalini M, d'Ettorre G, Venditti M, Vullo V, Orsi GB. A seven-year prospective study on spondylodiscitis: epidemiological and microbiological features. Infection. 2010 Apr;38(2):102-7. DOI: 10.1007/s15010-009-9340-8
[28] Huang S, Kappel AD, Peterson C, Chamiraju P, Rajah GB, Moisi MD. Cervical spondylodiscitis caused by Candida albicans in a non-immunocompromised patient: A case report and review of literature. Surg Neurol Int. 2019 Aug 2;10:151. doi: 10.25259/SNI_240_2019
[29] El Khoury C, Younes P, Hallit R, Okais N, Matta MA. Candida glabrata spondylodiscitis: A case report. J Infect Dev Ctries. 2018 Feb;12(2.1):32S. DOI: 10.3855/jidc.10062
[30] Yang H, Shah AA, Nelson SB, Schwab JH. Fungal spinal epidural abscess: a case series of nine patients. Spine J. 2019 Mar;19(3):516-22. DOI: 10.1016/j.spinee.2018.08.001
[31] Boyd B, Pratt T, Mishra K. Fungal Lumbosacral Osteomyelitis After Robotic-Assisted Laparoscopic Sacrocolpopexy. Female Pelvic Med Reconstr Surg. 2018;24(6):e46-e48. DOI: 10.1097/SPV.0000000000000612
[32] Kroot EJ, Wouters JM. An unusual case of infectious spondylodiscitis. Rheumatology (Oxford). 2007 Aug;46(8):1296. DOI: 10.1093/rheumatology/kem110
[33] Grimes CL, Tan-Kim J, Garfin SR, Nager CW. Sacral colpopexy followed by refractory Candida albicans osteomyelitis and discitis requiring extensive spinal surgery. Obstet Gynecol. 2012 Aug;120(2 Pt 2):464-8. DOI: 10.1097/AOG.0b013e318256989e
[34] Salzer HJ, Rolling T, Klupp EM, Schmiedel S. Hematogenous dissemination of Candida dubliniensis causing spondylodiscitis and spinal abscess in a HIV-1 and HCV-coinfected patient. Med Mycol Case Rep. 2015 Jun;8:17-20. DOI: 10.1016/j.mmcr.2015.02.001
[35] de Matos IG, do Carmo G, Araujo ML. Spondylodiscitis by Candida albicans. Infection. 1998;26(3):195-6. DOI: 10.1007/BF02771856
[36] Jorge VC, Cardoso C, Noronha C, Simões J, Riso N, Vaz Riscado M. 'Fungal spondylodiscitis in a non-immunocompromised patient'. BMJ Case Rep. 2012 Mar 8;2012:bcr1220115337. DOI: 10.1136/bcr.12.2011.5337
[37] Zou MX, Peng AB, Dai ZH, Wang XB, Li J, Lv GH, Deng YW, Wang B. Postoperative initial single fungal discitis progressively spreading to adjacent multiple segments after lumbar discectomy. Clin Neurol Neurosurg. 2015 Jan;128:101-6. DOI: 10.1016/j.clineuro.2014.11.012
[38] Zhong Y, Huang Y, Zhang D, Chen Z, Liu Z, Ye Y. Isolated cryptococcal osteomyelitis of the sacrum in an immunocompetent patient: a case report and literature review. BMC Infect Dis. 2023 Feb;23(1):116. DOI: 10.1186/s12879-023-08066-6
[39] Ur-Rahman N, Jamjoom ZA, Jamjoom A. Spinal aspergillosis in nonimmunocompromised host mimicking Pott's paraplegia. Neurosurg Rev. 2000 Jun;23(2):107-11. DOI: 10.1007/pl00021703
[40] Vaishya S, Sharma MS. Spinal Aspergillus vertebral osteomyelitis with extradural abscess: case report and review of literature. Surg Neurol. 2004 Jun;61(6):551-5; discussion 555. DOI: 10.1016/j.surneu.2003.06.005
[41] Sethi S, Siraj F, Kalra K, Chopra P. Aspergillus vertebral osteomyelitis in immunocompetent patients. Indian J Orthop. 2012 Mar;46(2):246-50. DOI: 10.4103/0019-5413.93693
[42] Eisen DP, MacGinley R, Christensson B, Larsson L, Woods ML. Candida tropicalis vertebral osteomyelitis complicating epidural catheterisation with disease paralleled by elevated D-arabinitol/L-arabinitol ratios. Eur J Clin Microbiol Infect Dis. 2000 Jan;19(1):61-3. DOI: 10.1007/s100960050013
[43] Derkinderen P, Bruneel F, Bouchaud O, Regnier B. Spondylodiscitis and epidural abscess due to Candida albicans. Eur Spine J. 2000 Feb;9(1):72-4. DOI: 10.1007/s005860050013
[44] Sebastiani GD, Galas F. Spondylodiscitis due to Candida tropicalis as a cause of inflammatory back pain. Clin Rheumatol. 2001;20(6):435-7. DOI: 10.1007/s100670170011
[45] Rachapalli SM, Malaiya R, Mohd TA, Hughes RA. Successful treatment of Candida discitis with 5-flucytosine and fluconazole. Rheumatol Int. 2010 Sep;30(11):1543-4. DOI: 10.1007/s00296-009-1215-x
[46] Rössel P, Schønheyder HC, Nielsen H. Fluconazole therapy in Candida albicans spondylodiscitis. Scand J Infect Dis. 1998;30(5):527-30. DOI: 10.1080/00365549850161601
[47] Pemán J, Jarque I, Bosch M, Cantón E, Salavert M, de Llanos R, Molina A. Spondylodiscitis caused by Candida krusei: case report and susceptibility patterns. J Clin Microbiol. 2006 May;44(5):1912-4. DOI: 10.1128/JCM.44.5.1912-1914.2006
[48] Jiang Z, Wang Y, Jiang Y, Xu Y, Meng B. Vertebral osteomyelitis and epidural abscess due to Aspergillus nidulans resulting in spinal cord compression: case report and literature review. J Int Med Res. 2013 Apr;41(2):502-10. DOI: 10.1177/0300060513476432
[49] Chia SL, Tan BH, Tan CT, Tan SB. Candida spondylodiscitis and epidural abscess: management with shorter courses of anti-fungal therapy in combination with surgical debridement. J Infect. 2005 Jul;51(1):17-23. DOI: 10.1016/j.jinf.2004.08.020
[50] Ackerman G, Bayley JC. Candida albicans osteomyelitis in a vertebral body previously infected with Serratia marcescens. Spine (Phila Pa 1976). 1990 Dec;15(12):1362-3. DOI: 10.1097/00007632-199012000-00024
[51] van Ooij A, Beckers JM, Herpers MJ, Walenkamp GH. Surgical treatment of aspergillus spondylodiscitis. Eur Spine J. 2000 Feb;9(1):75-9. DOI: 10.1007/s005860050014
[52] Ugarriza LF, Cabezudo JM, Lorenzana LM, Rodríguez-Sánchez JA. Candida albicans spondylodiscitis. Br J Neurosurg. 2004 Apr;18(2):189-92. DOI: 10.1080/02688690410001681091
[53] El-Zaatari MM, Hulten K, Fares Y, Baassiri A, Balkis M, Almashhrawi A, El-Zaatari FA. Successful treatment of Candida albicans osteomyelitis of the spine with fluconazole and surgical debridement: case report. J Chemother. 2002 Dec;14(6):627-30. DOI: 10.1179/joc.2002.14.6.627
[54] Friedman BC, Simon GL. Candida vertebral osteomyelitis: report of three cases and a review of the literature. Diagn Microbiol Infect Dis. 1987 Sep;8(1):31-6. DOI: 10.1016/0732-8893(87)90044-7
[55] Torres-Ramos FM, Botwin K, Shah CP. Candida spondylodiscitis: an unusual case of thoracolumbar pain with review of imaging findings and description of the clinical condition. Pain Physician. 2004 Apr;7(2):257-60.
[56] Pennisi AK, Davis DO, Wiesel S, Moskovitz P. CT appearance of Candida diskitis. J Comput Assist Tomogr. 1985;9(6):1050-4. DOI: 10.1097/00004728-198511000-00009
[57] Hennequin C, Bourée P, Hiesse C, Dupont B, Charpentier B. Spondylodiskitis due to Candida albicans: report of two patients who were successfully treated with fluconazole and review of the literature. Clin Infect Dis. 1996 Jul;23(1):176-8. DOI: 10.1093/clinids/23.1.176
[58] Mullins RF, Still JM Jr, Savage J, Davis JB, Law EJ. Osteomyelitis of the spine in a burn patient due to Candida albicans. Burns. 1993 Apr;19(2):174-6. DOI: 10.1016/0305-4179(93)90045-a
[59] Crane JK. Intrathecal spinal abscesses due to Candida albicans in an immunocompetent man. BMJ Case Rep. 2018 Mar 27;2018:bcr2017223326. DOI: 10.1136/bcr-2017-223326
[60] Kashimoto T, Kitagawa H, Kachi H. Candida tropicalis vertebral osteomyelitis and discitis. A case report and discussion on the diagnosis and treatment. Spine (Phila Pa 1976). 1986;11(1):57-61. DOI: 10.1097/00007632-198601000-00016
[61] Liu B, Qu L, Zhu J, Yang Z, Yan S. Histoplasmosis mimicking metastatic spinal tumour. J Int Med Res. 2017 Aug;45(4):1440-6. DOI: 10.1177/0300060517708530
[62] Lee JH, Chough CK, Choi SM. Late onset Candida albicans spondylodiscitis following candidemia: a case report. Korean J Med Mycol. 2017:117–21. DOI: 10.17966/KJMM.2017.22.3.117
[63] Kelesidis T, Tsiodras S. Successful treatment of azole-resistant Candida spondylodiscitis with high-dose caspofungin monotherapy. Rheumatol Int. 2012 Sep;32(9):2957-8. DOI: 10.1007/s00296-011-2121-6
[64] Bruns J, Hemker T, Dahmen G. Fungal spondylitis. A case of Torulopsis glabrata and Candida tropicalis infection. Acta Orthop Scand. 1986 Dec;57(6):563-5. DOI: 10.3109/17453678609014795
[65] Kulcheski ÁL, Graells XS, Benato ML, Santoro PG, Sebben AL. Fungal spondylodiscitis due to Candida albicans: an atypical case and review of the literature. Rev Bras Ortop. 2015;50(6):739-42. DOI: 10.1016/j.rboe.2015.10.005
[66] Neale TJ, Muir JC, Mills H, Horne JG, Jones MR. Candida albicans vertebral osteomyelitis in chronic renal failure. Postgrad Med J. 1987 Aug;63(742):695-8. DOI: 10.1136/pgmj.63.742.695
[67] Relvas-Silva M, Pinho AR, Vital L, Leão B, Sousa AN, Carvalho AC, Veludo V. Azole-resistant Candida albicans Spondylodiscitis After Bariatric Surgery: A Case Report. JBJS Case Connect. 2020;10(3):e19.00618. DOI: 10.2106/JBJS.CC.19.00618
[68] Takagi Y, Yamada H, Ebara H, Hayashi H, Kidani S, Okamoto S, Nakamura Y, Kitano Y, Kagechika K, Demura S, Ueno T, Shimozaki K, Tsuchiya H. Aspergillus terreus spondylodiscitis following an abdominal stab wound: a case report. J Med Case Rep. 2019 Jun;13(1):172. DOI: 10.1186/s13256-019-2109-5
[69] Bhat SN, Kundangar R, Ampar N, Banerjee B, Udupa CBK, Saravu K. Cryptococcal spondylodiscitis in a non-HIV patient with CD4 lymphocytopenia. J Taibah Univ Med Sci. 2021 Jun;16(3):470-5. DOI: 10.1016/j.jtumed.2021.01.007
[70] Edwards JE, Turkel SB, Elder HA, Rand RW, Guze LB. Hematogenous candida osteomyelitis. Report of three cases and review of the literature. Am J Med. 1975 Jul;59(1):89-94. DOI: 10.1016/0002-9343(75)90325-3
[71] Dai G, Wang T, Yin C, Sun Y, Xu D, Wang Z, Luan L, Hou J, Li S. Aspergillus spondylitis: case series and literature review. BMC Musculoskelet Disord. 2020 Aug;21(1):572. DOI: 10.1186/s12891-020-03582-x
[72] Williams RL, Fukui MB, Meltzer CC, Swarnkar A, Johnson DW, Welch W. Fungal spinal osteomyelitis in the immunocompromised patient: MR findings in three cases. AJNR Am J Neuroradiol. 1999 Mar;20(3):381-5.
[73] Lopes A, Albanez Andrade R, Gonelli Andrade R, Berardo Pessoa Zirpoli B, Burgos Souto Maior A, Aguiar de Lima Silva G, et al. Candida tropicalis spondylodiscits in an immunocompetent host: a case report and literature review. Arq Bras Neurocir. 2021;40(04):e412-e416. DOI: 10.1055/s-0041-1735800
[74] Er H, Yilmaz NÖ, Sandal E, Şenoğlu M. A case of candida spondylodiscitis in an immunocompetent patient. Ann Clin Anal Med. 2020;11(Suppl_01):85-8. [cited 2024 Feb 20]. DOI: 10.4328/ACAM.20103
[75] Sugar AM, Saunders C, Diamond RD. Successful treatment of Candida osteomyelitis with fluconazole. A noncomparative study of two patients. Diagn Microbiol Infect Dis. 1990;13(6):517-20. DOI: 10.1016/0732-8893(90)90084-9
[76] Rashid MH, Hossain MN, Ahmed N, Kazi R, Ferini G, Palmisciano P, Scalia G, Umana GE, Hoz SS, Chaurasia B. Aspergillus spinal epidural abscess: A case report and review of the literature. J Craniovertebr Junction Spine. 2022 Apr-Jun;13(2):204-11. DOI: 10.4103/jcvjs.jcvjs_35_22
[77] Yoon KW, Kim YJ. Lumbar Aspergillus osteomyelitis mimicking pyogenic osteomyelitis in an immunocompetent adult. Br J Neurosurg. 2015 Apr;29(2):277-9. DOI: 10.3109/02688697.2014.957648
[78] Upadhyay AS, Bapat MR, Patel BK, Gujral A. Postoperative fungal discitis in immune-competent patients: a series of five patients. Indian Spine J. 2020 Dec;3(2):243-9. DOI: 10.4103/isj.isj_41_19
[79] Seravalli L, Van Linthoudt D, Bernet C, de Torrenté A, Marchetti O, Porchet F, Genné D. Candida glabrata spinal osteomyelitis involving two contiguous lumbar vertebrae: a case report and review of the literature. Diagn Microbiol Infect Dis. 2003 Feb;45(2):137-41. DOI: 10.1016/s0732-8893(02)00497-2
[80] Schilling A, Seibold M, Mansmann V, Gleissner B. Successfully treated Candida krusei infection of the lumbar spine with combined caspofungin/posaconazole therapy. Med Mycol. 2008 Feb;46(1):79-83. DOI: 10.1080/13693780701552996
[81] Oichi T, Sasaki S, Tajiri Y. Spondylodiscitis concurrent with infectious aortic aneurysm caused by Candida tropicalis: a case report. J Orthop Surg (Hong Kong). 2015 Aug;23(2):251-4. DOI: 10.1177/230949901502300230
[82] Herzog W, Perfect J, Roberts L. Intervertebral diskitis due to Candida tropicalis. South Med J. 1989 Feb;82(2):270-3. DOI: 10.1097/00007611-198902000-00029
[83] Shaikh BS, Appelbaum PC, Aber RC. Vertebral disc space infection and osteomyelitis due to Candida albicans in a patient with acute myelomonocytic leukemia. Cancer. 1980 Mar;45(5):1025-8. DOI: 10.1002/1097-0142(19800301)45:5<1025::aid-cncr2820450532>3.0.co;2-i
[84] Hadjipavlou AG, Mader JT, Nauta HJ, Necessary JT, Chaljub G, Adesokan A. Blastomycosis of the lumbar spine: case report and review of the literature, with emphasis on diagnostic laboratory tools and management. Eur Spine J. 1998;7(5):416-21. DOI: 10.1007/s005860050100
[85] Savall F, Dedouit F, Telmon N, Rougé D. Candida albicans spondylodiscitis following an abdominal stab wound: forensic considerations. J Forensic Leg Med. 2014 Mar;23:1-3. DOI: 10.1016/j.jflm.2013.12.027
[86] Duplan P, Memon MB, Choudhry H, Patterson J. A Rare Case of Candida parapsilosis Lumbar Discitis With Osteomyelitis. Cureus. 2022 Jun 15;14(6):e25955. DOI: 10.7759/cureus.25955
[87] Werner BC, Hogan MV, Shen FH. Candida lusitaniae discitis after discogram in an immunocompetent patient. Spine J. 2011 Oct;11(10):e1-6. DOI: 10.1016/j.spinee.2011.09.004
[88] Dailey NJ, Young EJ. Candida glabrata spinal osteomyelitis. Am J Med Sci. 2011 Jan;341(1):78-82. DOI: 10.1097/MAJ.0b013e3181f6c6ea
[89] Fogarty M. Candidial osteomyelitis: a case report. Aust N Z J Surg. 1983 Apr;53(2):141-3. DOI: 10.1111/j.1445-2197.1983.tb02415.x
[90] Holzman RS, Bishko F. Osteomyelitis in heroin addicts. Ann Intern Med. 1971 Nov;75(5):693-6. DOI: 10.7326/0003-4819-75-5-693
[91] Chen CH, Chen WL, Yen HC. Candida albicans lumbar spondylodiscitis in an intravenous drug user: a case report. BMC Res Notes. 2013 Dec;6:529. DOI: 10.1186/1756-0500-6-529
[92] Rieneck K, Hansen SE, Karle A, Gutschik E. Microbiologically verified diagnosis of infectious spondylitis using CT-guided fine needle biopsy. APMIS. 1996 Oct;104(10):755-62. DOI: 10.1111/j.1699-0463.1996.tb04939.x
[93] Gagliano M, Marchiani C, Bandini G, Bernardi P, Palagano N, Cioni E, Finocchi M, Bellando Randone S, Moggi Pignone A. A rare case of Candida glabrata spondylodiscitis: case report and literature review. Int J Infect Dis. 2018 Mar;68:31-35. DOI: 10.1016/j.ijid.2018.01.003
[94] Hayes WS, Berg RA, Dorfman HD, Freedman MT. Case report 291. Diagnosis: Candida discitis and vertebral osteomyelitis at L1-L2 from hematogenous spread. Skeletal Radiol. 1984;12(4):284-7. DOI: 10.1007/BF00349511
[95] Alvarenga JA, Martins DE, Kanas M, Elizeche HG, Dell'Aquila AM, Fernandes EA, Wajchenberg M, Puertas EB. Paracoccidioidomycosis in the spine: case report and review of the literature. Sao Paulo Med J. 2016;134(3):263-267. DOI: 10.1590/1516-3180.2015.02691801
[96] Munk PL, Lee MJ, Poon PY, O'Connell JX, Coupland DB, Janzen DL, Logan PM, Dvorak MF. Candida osteomyelitis and disc space infection of the lumbar spine. Skeletal Radiol. 1997 Jan;26(1):42-6. DOI: 10.1007/s002560050189
[97] Wang C, Zhang L, Zhang H, Xu D, Ma X. Sequential endoscopic and robot-assisted surgical solutions for a rare fungal spondylodiscitis, secondary lumbar spinal stenosis, and subsequent discal pseudocyst causing acute cauda equina syndrome: a case report. BMC Surg. 2022 Jan;22(1):34. DOI: 10.1186/s12893-022-01493-3
[98] Overgaauw AJC, de Leeuw DC, Stoof SP, van Dijk K, Bot JCJ, Hendriks EJ. Case report: Candida krusei spondylitis in an immunocompromised patient. BMC Infect Dis. 2020 Oct;20(1):739. DOI: 10.1186/s12879-020-05451-3
[99] Supreeth S, Al Ghafri KA, Jayachandra RK, Al Balushi ZY. First Report of Candida auris Spondylodiscitis in Oman: A Rare Presentation. World Neurosurg. 2020 Mar;135:335-8. DOI: 10.1016/j.wneu.2019.09.021
Attachments
| Attachment 1 | Table 1: All studies included in the review (Attachment1_dgkh000624.pdf, application/pdf, 738.21 KBytes) |

