Training supported by simulated persons to promote the development of specific communication skills in advance care planning
Kornelia Götze 1Stefanie Otten-Marré 2
Barbara Loupatatzis 3
Jürgen in der Schmitten 1
1 University of Duisburg-Essen, Medical Faculty, Institute of Family Medicine & General Practice, Essen, Germany
2 University Hospital Düsseldorf, Centre for Health and Society (chs), Institute of General Practice & General Practice, Düsseldorf, Germany
3 GZO Wetzikon Hospital, Palliative Care Team, Wetzikon, Switzerland
Abstract
Objectives: Advance care planning (ACP) has been conceived to ensure that patients who are unable to consent are treated in consistence with their well-informed, predetermined preferences. At an individual level, standardised conversations are offered by specifically qualified healthcare professionals (ACP facilitators). Internationally, there is considerable variability with regard to ACP qualifications. This article describes how ACP facilitators are trained in role plays employing simulated persons (SPs) in accordance with the standards of two professional societies.
Methods: ACP experts developed ten roles in cooperation with an SP coach (director) based on real ACP conversations. The emotional and mental world of the role, ACP-relevant facts such as previous experience in the medical context, and aids for acting were developed, taking into account the central challenges in ACP conversations. To ensure standardisation, the SPs rehearsed in a structured manner and received feedback training. Microteaching techniques were developed for the facilitator training.
Results: Feedback skills and openness towards the topics of serious illness, dying and death are required for the SP to be suitable. Since 2017, ACP facilitator training has taken place in small groups of four participants, one SP and one qualified ACP coach. The required framework is described in detail.
Conclusion: SP-supported training is a decisive improvement for the teaching and assessment of the highly complex ACP-facilitation skills and attitudes. Planning and implementation place high demands on SP and ACP coaches who also require specific qualifications.
Keywords
teaching methods, simulation patient/person, training for complex communication skills, advance care planning
1. Introduction
1.1. Advance care planning
Advance care planning (ACP) aims to ensure that patients who are unable to consent [1] receive care consistent with their well-informed predetermined preferences [2], [3]. This requires comprehensive developments in the healthcare system at an individual, institutional and regional level (ACP programme) [4]. The institutional and regional implementation of the ACP programme must ensure that the preferences of the person incapable of decision-making are known and honoured in the event of severe illness. At the individual level, a multi-stage outreach offer to have an ACP conversation is made by a qualified specialist, a so-called ACP facilitator. The conversation can lead to a meaningful advance directive.
1.2. ACP facilitator qualification meeting the standards of ACP Germany and ACP Swiss
Internationally, there have been training programmes for ACP facilitators since the 1990s [5], but only a few of these have been implemented with simulated persons (SP) (e.g. to tatou reo – New Zealand [6]); there is no systematic survey on this subject. The joint standard of the professional societies ACP Germany (ACP-D) [7] and ACP Swiss [8] for an eight-day ACP facilitator qualification, on which this article is based, was developed in 2017/18 on the basis of the respective national predecessors [7], [9], [10], [11] and internationally established ACP programmes [5], [12] (see figure 1 [Fig. 1] and attachment 1 [Att. 1]). The standard draws from experience in SP-supported teaching “breaking bad news” to medical students with similar requirements regarding communication skills [13], [14].
Figure 1: Overview of the 8-day ACP facilitator qualification from ACP Deutschland e.V. following the introduction of SP-supported training in 2017. 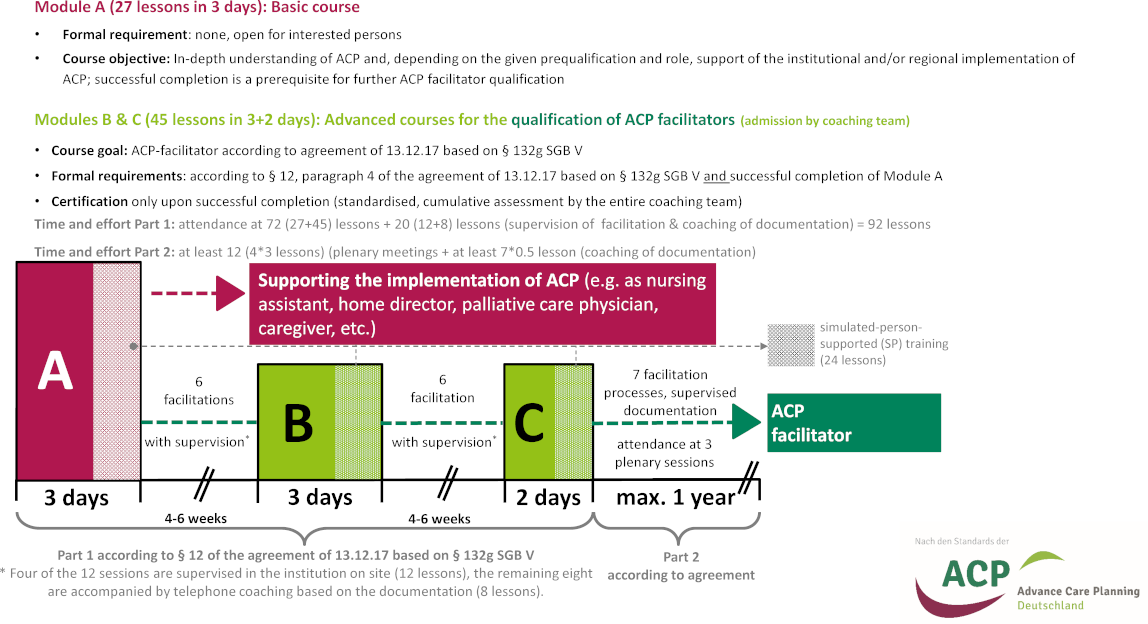
Further details of the ACP facilitator qualification, such as the daily schedule, can be found in Götze et al. 2022 [8], additional file 1.
Before the introduction of SP training, there were already participants and demonstration role plays (see table 1). With the introduction of the SP-supported training, the course was divided into three modules in order to intensify the facilitation between the modules in practical application.
ACP: advance care planning, TU: teaching units (45 minutes), SGB: German Social Security Code, SP: simulated person.
This figure was originally published in Götze K et al. 2022 [8], additional file 1. © Götze et al. https://creativecommons.org/licenses/by/4.0/
The four sections in the ACP conversation described below are first introduced theoretically during the ACP facilitator qualification and then practiced with SP and in real life (see attachment 1 [Att. 1], table S1b).
ACP facilitation for the planning of treatment goals and possible limits in future life-threatening situations in advance touch on sensitive and existential issues [15], [16]. Therefore, exploration of the individual's underlying treatment goal by discussing personal “attitudes towards life, dying and serious illness” form the basis for the medical preferences in the ACP process. Beyond that, specific care preferences are determined for acute emergencies [17], for hospital treatments in case of decisional incapacity of uncertain duration [18], and for treatments in case of permanent loss of decision-making capacity. For persons incapable of decision making the surrogates are empowered to record the presumed care preferences of the person concerned for emergencies and for the event of a future deterioration of their condition [8], [19] (see attachment 1 [Att. 1], table S1b).
Conducting the conversation requires a combination of a particularly sensitive, open-ended approach and a certain degree of lead so that the people engaged in advance care planning can clarify the key issues for themselves. This sensitive approach can include, touching on taboo subjects as well as enduring and carefully channeling the associated strong emotions in order to enable valid advance care planning [20].
The teams dealing with a medical crisis must also be able to rely on the fact that the documentation of these conversations is a reliable reflection of the person's care preferences (validity). By implication, this means that the participants should only pass the qualification and be certified accordingly if the required skills (see attachment 2 [Att. 2]) have been confirmed by a reliable skill and performance assessment (see attachment 3 [Att. 3]) as part of the ACP facilitator qualification.
1.3. SP-supported training to improve communication skills
Role-play is ideal for deepening communicative skills since these cannot be reliably built up through mere listening or interactive learning [21]. The strength of participant role-play lies in the change of perspective. The additional use of SP-supported role-play in the ACP facilitator qualification (see table 1 [Tab. 1] and table 2 [Tab. 2]) makes possible
- to reliably anchor standard situations in the ACP facilitation process (especially challenges) in the curriculum [22],
- to include the option of going back to a specific point in the conversation with pinpoint accuracy in order to repetitively practice particularly challenging aspects of conducting the ACP conversation [23],
- to give participants a sense of achievement [23], and
- to perform a cumulative skills assessment with a standardised level of difficulty (see table 2 [Tab. 2]) [24].
Table 1: Role of SP-supported training in the acquisition of ACP facilitator skills
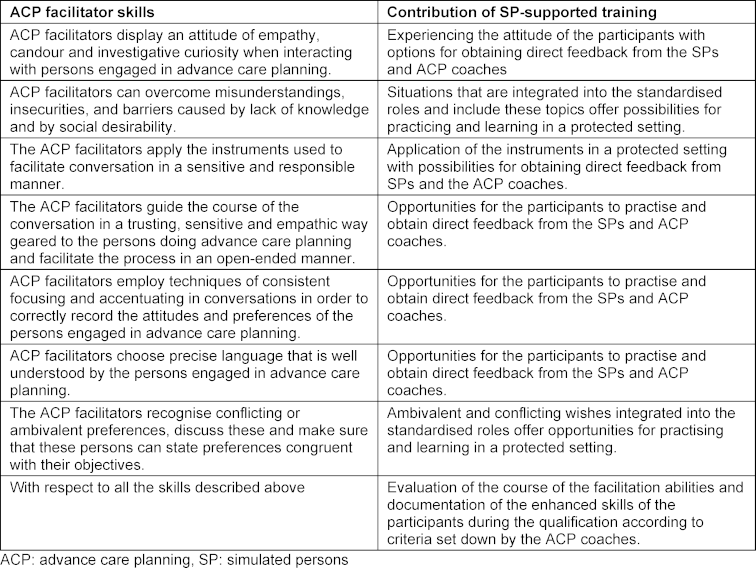
Table 2: Benefits of standardised SP at a glance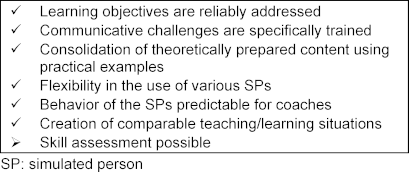
When training communicative skills, SPs portray people in various scenarios [13]: from short medical histories to complex, emotionally charged conversational situations in which the attitude, preferences, biography and fate of the presented patient-role may be revealed [25].
As different as the simulated conversations are, the acting challenges for the SP also vary. While the simpler conversations require the most accurate possible recapitulation of the role's medical history as well as flexible interaction with and spontaneous reactions to the other person, more complex conversational situations require, for example, the truthful portrayal of emotions and the inner attitude of the role [26]. In addition, corresponding body language must be used and the conversational situations to be called up must be repeatable and standardised [26].
The scripts of the respective role and the rehearsals of the SP must be designed accordingly. In roles that are intended to train more complex communication skills, medical details take a back seat to life story, thoughts and emotions and only form a thematic framework for the respective role [27]. Moreover, since the trained SPs are medical laypersons, it would be unhelpful to focus on medical details in the role script. Rather, inner images and memories of patients regarding their symptoms and illnesses as well as challenges and effects in everyday life give the actors a deeper impression of the existential framework and the experience of the illness from the perspective of the roles [26].
Another strength of SP-supported training is the professional feedback provided by well-trained SPs from the perspective of the role directly to those conducting the conversation [13]. It is very impressive to receive a description of how the patient perceived the conversation from the experience of the patient role and what the SP would have wished for in the role. This can support the participants’ self-reflection.
2. SP-supported training in the qualification of ACP facilitators
The following is a detailed description of SP-supported training, from the conception of the roles and rehearsal work to the organisation of the course and the actual implementation of the SP-supported training.
2.1. Eligibility of the SP
Professional actors and trained laypersons, some of whom already have experience as SPs in teaching, are employed for SP-supported training as part of the ACP facilitator qualification. In order to develop eligibility criteria for SPs, comparative observations and structured exchanges were conducted in the context of five ACP facilitator qualifications in 2017 and 2018 by ten ACP coaches and three SP coaches [28]. There were no indications that the professional actors were better able to cope with the requirements than were the well trained laypersons.
Sometimes the professional actors were able to access emotions and body language more easily and develop the role more quickly. For a good performance as an SP, however, spontaneous interaction with the participant and the ability to give detailed feedback are crucial in addition to classical acting. An openness to allow, endure and reflect on the taboo subjects of death and dying has proven to be central to these interactions. This openness is related more to personality than to expertise as an actor.
2.2. Conception and rehearsal of the roles
Phenomena and challenges frequently encountered in real ACP faciliations were identified for the design of the roles in order to train them under secure course conditions with the aim of being able to put what has been learnt into practice in new and modified everyday situations [22]. Ten roles were derived based on real people engaged in advance care planning conversations (see attachment 4 [Att. 4]).
Comparatively extensive (~ 10,000 words) role scripts were developed for the ten characters by ACP coaches in collaboration with an SP coach.
The structure of the script was based on the course of the standardised ACP conversation. In the role scripts, the biography and the emotional, life and mental situation of the persons to be simulated were formulated in general as well as attitudes, opinions, previous experiences, thoughts and feelings that are of particular importance for the topics of advance care planning.
In order to facilitate access to the role, various technical acting aids were included in the role scripts. These include, for example, inner monologues and non-verbal and verbal cues such as posture or voice modulation (see figure 2 [Fig. 2]).
Figure 2: Exemplary sections from the role scripts for the simulated persons in the ACP facilitator qualification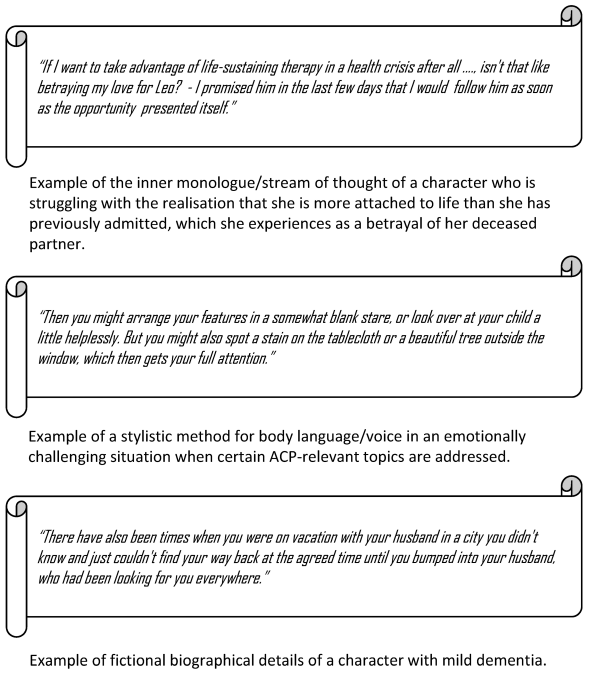
The scripts were refined in an iterative process as part of the rehearsal work and SP performances in order to ensure standardisation when incorporating future SPs (see table 2 [Tab. 2]).
Facts relevant for advance care planning (e.g. illnesses experienced by oneself or others) or medical facts were combined with their subjective significance for the particular role in order to achieve the most homogeneous interpretation possible by different SPs. This detailed role representation permitted a high degree of standardisation of the roles, even over long periods of time (see table 2 [Tab. 2]).
2.2.1. Preparation for the rehearsal
Ten SPs from the SP pool established for teaching purposes at Heinrich Heine University in Düsseldorf (CoMeD) were rehearsed for the ACP facilitator qualifications. The SPs were briefed in advance about the project and the task to be completed; in particular, the sensitive topics of illness, death and dying were discussed with the SPs in this protected setting. The role script, which was sent out well in advance of the rehearsals, was prepared independently by the SPs. All SPs, the SP coach and at least one ACP coach were requested for the rehearsal days. Half a rehearsal day per role proved to be useful.
2.2.2. On-site rehearsal of the SP
During the rehearsals, there was an exchange and reflection on the respective role. The group created an identity card (IC) for the roles of the persons undertaking an advance care planning conversation on a flipchart, on which the most important character traits were recorded as well as possibilities for translation into body language and expression [29]. This IC is a concise summary of the role and its portrayal and has since supported the SPs in evoking the character during the ACP facilitator courses. The core component of the rehearsals was practicing the role in the conversation. For this purpose, an ACP coach was available to support the SPs as a conversational partner. The performance was then reflected on together. Additions and corrections were discussed and recorded in the script and the IC. In addition, acting assistance was given for the performance or for getting into and out of the role, and giving feedback after the conversation with the SPs was practised.
Joint development and rehearsal of the roles improved the standardisation (see table 2 [Tab. 2]) since the SP colleagues served as orientation [30].
2.3. Organisation before and during the ACP workshops with SP
When planning the ACP facilitator qualification, additional time-consuming tasks must be taken into account when adding SPs, for which special resources must be planned. For example, SPs must be contacted and coordinated so that one SP is available for each small group of four participants at the appropriate times in addition to the ACP coach. In addition, an SP coach should be available to the SPs during and after the assignments for questions about the roles and for debriefing, even at short notice, at least by telephone or online.
Rotation plans drawn up in advance by the ACP course centres can ensure that the participants ideally always experience the same SP in the same roles in the course of the qualification, as the roles are accompanied by several ACP conversation sections during the course. The level of difficulty also increases from role to role depending on the ACP conversation section to be trained. In these rotation plans, the SPs are clearly assigned to the rooms and people in order to ensure that the course runs smoothly.
Prior to the course, the SPs receive a letter containing all relevant information on times, locations and rotations.
If possible, the SPs should be provided with a separate room on site for preparation, props and breaks. They can prepare there and get into and out of their roles after their performances. This retreat room also helps to separate the real people (SPs) from the roles that the SPs embody for the participants.
With regard to the SPs, it should be borne in mind that the simulations are a challenge for many participants, especially at the beginning, e.g. situations they have experienced themselves that were characterised by serious illnesses or the loss of loved ones can become present again through the simulation of the ACP conversation, as we have often experienced in the courses. Experience has shown that these challenges for the participants in the new role of ACP facilitator can sometimes lead to emotionally charged (possibly even hostile) behaviour towards the SPs, which can be stressful for everyone. In our experience, special attention by ACP and SP coaches is therefore necessary to enable these situations to be worked through not only with the participants, but also with the SPs. It has proven to be wise to offer the SPs a debriefing (see above) with an ACP coach with SP experience from the course and the SP coach (by telephone/online if necessary) directly after their performance. Experience has shown that continuous quality assurance, provided by SP coaches supporting the ACP facilitator courses on site, is necessary after two to three performances, at new course centres, and during the introduction of new SPs or new roles [13] in order to maintain standardisation.
2.4. Implementation of the SP-supported teaching lessons
The SP role-play takes place in small groups of a maximum of four participants, with each group guided by a qualified ACP coach.
Before the SP-supported training begins, the sitting positions, i.e. the setting, are organised. It is essential that the participants are actively encouraged by the coach to adjust their own sitting positions and those of the simulated person(s) engaged in an advance care planning conversation at their own discretion and to place the ACP coach according to their preferences. Through this leeway and the associated responsibility, the participants learn to develop an awareness of the importance of the setting. Both the needs of the ACP facilitator and those of the planning person (client) need and deserve to be considered. The other participants are given observation tasks (e.g. observing verbal and non-verbal communication).
After clarifying any open questions from the participant who is now conducting the ACP conversation, the available time and the rules of microteaching, the simulation begins. With a clear, pre-agreed signal, the coach has the option of interrupting the conversation for a microteaching unit. During the interruption, the SPs have the task of preserving their emotions from the previous minutes of the conversation as far as possible so that the simulation can be resumed seamlessly at a point determined by the coach and participants.
Before continuing the simulation, the ACP coach ensures that the SP is aware of the (new) starting point and is ready. This is often done non-verbally. The simulation is continued at a clear signal from the coach.
At the end of a simulation, the participants are debriefed and the SP and coach give feedback to the participants. The observations of the other participants are included in the feedback.
2.4.1. Microteaching
Microteaching (also described as Rapid Cycle Deliberate Practice [31]) in the sense used here means working closely on the course of the conversation, what is said and what is perceived; there are more frequent interruptions instead of focussing on the flow of the conversation and feedbacking a wrap-up at the end. This helps to prevent a cumulating list of detailed feedback especially in the case of inexperienced ACP facilitators, the processing of which would be overwhelming and remain incomplete. Above all, the classic two-part role-play format (=longer simulation phase followed by critical discussion) lacks the opportunity to directly try out alternative behaviour for a specific situative detail and possibly experience a sense of achievement.
The technique of microteaching has proven its worth in order to make optimum use of the limited time available for simulation training and to give participants both a feeling of self-efficacy through successful repetition and the steepest possible learning curve. Microteaching also makes it possible to identify participants who find the task of ACP faciliation too challenging or for whom it is not suitable as part of the skills assessment and self-reflection.
On the other hand, microteaching has the disadvantage that the flow of conversation is repeatedly interrupted; in our experience, participants can occasionally become so irritated by this that they are no longer able to continue the role-play. It is the task of the ACP coaches to recognise such irritation as early as possible and to make use of the didactic instrument of microteaching (see table 3 [Tab. 3]) judiciously. In individual cases, an unscheduled switch of the participant in the role of ACP facilitator can be useful in order to relieve the participant irritated by the interruptions.
Table 3: Techniques of microteaching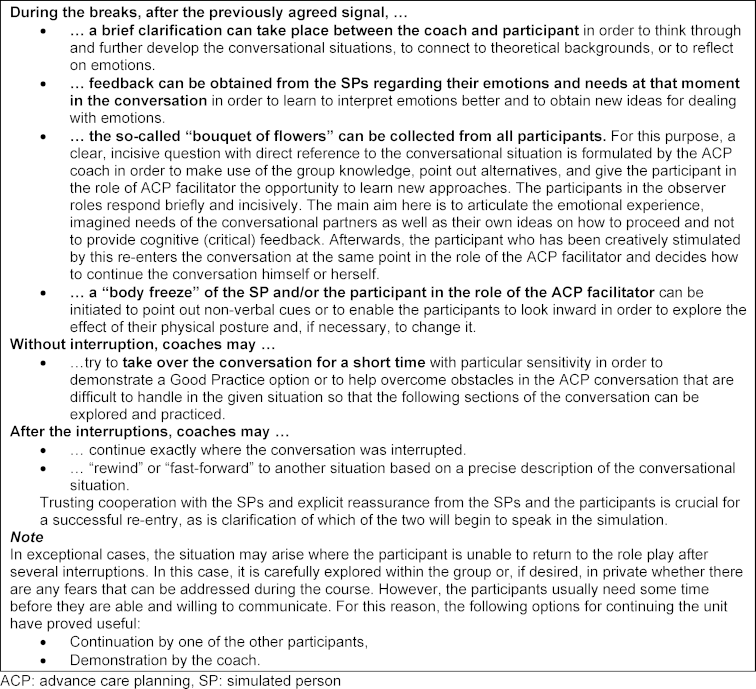
The techniques listed in table 3 [Tab. 3] have become established in the ACP facilitator qualifications for organising microteaching, and go beyond the techniques known to the authors from the literature [31], [32].
2.5. Standardisation during the creation of multiple SP pools
After the first SP pool for ACP facilitator qualifications meeting ACP-D standards was established in Düsseldorf, it became necessary to create SP pools for ACP facilitator qualifications at other ACP facilitator course centres (including centres in Zurich, Munich, Frankfurt, Göttingen and Marburg) as demand for courses increased. The testing of the local SPs for the roles was carried out in mutual consultation with the support of the Düsseldorf SP coach (co-author of this article: SOM) with the aim of transferring the know-how developed in Düsseldorf and realising a Germany-wide standardisation of the SPs (see table 2 [Tab. 2]) and thus also of the ACP facilitator qualification [30]. The regional SP coaches are responsible for coordinating and monitoring the performances as part of the ACP facilitator qualification.
3. Conclusions
SP-supported trainings are a decisive improvement for the teaching and evaluation of the highly complex ACP facilitator skills and their attitude. In addition, according to the many years of experience gained by coaches certified by ACP Germany or ACP Swiss, it cannot be replaced by any other methodological format for this particular qualification. Developing the roles, selecting and testing the SPs, organising the assignments and conducting the simulation training in small groups places high demands not only on the SPs, but also on the ACP coaches in particular, who require their own specific qualifications in this regard [8], [33], [34].
Notes
Authors’ ORCIDs
- Kornelia Götze: [0000-0001-8134-7521]
- Stefanie Otten-Marré: [0009-0002-7064-6109]
- Barbara Loupatatzis: [0009-0006-7276-5944]
- Jürgen in der Schmitten: [0000-0001-5960-1511]
Funding
The development of the SP training was funded by the Federal Ministry of Health as part of the project “Promotion of the implementation of §132g SGB V according to HPG” under the reference no. ZMVI1-2516FSB801.
Secondary publication
This manuscript is also published in a slightly adapted version and without figures, tables and supplements in Praxisbuch Advance Care Planning. Behandlungsentscheidungen gemeinsam vorausplanen (in print) [35].
Acknowledgements
I. Karzig, D. Otto and Prof. Dr. T. Krones from the ACP working group of University Hospital Zurich as well as Prof. Dr. Dr. B. Feddersen, Prof. Dr. G. Marckmann and Dr. S. Petri from the ACP Germany working group “qualification”, with whose support the qualification for ACP facilitation was designed. Prof. Dr. H. Stanze for her support in writing a role script (inclusion assistance). All other ACP coaches who carry out the ACP facilitator qualifications according to these standards.
Competing interests
Barbara Loupatatzis, Jürgen in der Schmitten and Kornelia Götze are ACP coaches and received fees for conducting ACP qualifications, lectures or workshops on ACP. Jürgen in der Schmitten was (2011-2021) and Kornelia Götze is (since 08/2021) treasurer of the international professional association Advance Care Planning international e.V. Jürgen in der Schmitten (since 02/2017) and Kornelia Götze (since 06/2021) are board members of Advance Care Planning Deutschland e.V. Barbara Loupatatzis receives fees for the qualification of SPs in the context of ACP-Swiss e.V. qualifications. Stefanie Otten-Marré receives fees for the coordination and qualification of SPs as part of ACP qualifications. Translated with DeepL.com (free version)
References
[1] Hinweise und Empfehlungen der Bundesärztekammer zum Umgang mit Zweifeln an der Einwilligungsfähigkeit bei erwachsenen Patienten. Dtsch Arztebl. 2019;116(22):A-1133, B-933, C-921.[2] Sudore RL, Lum HD, You JJ, Hanson LC, Meier DE, Pantilat SZ, Matlock DD, Rietjens JA, Korfage IJ, Ritchie CS, Kutner JS, Teno JM, Thomas J, McMahan RD, Heyland DK. Defining Advance Care Planning for Adults: A Consensus Definition From a Multidisciplinary Delphi Panel. J Pain Symptom Manage. 2017;53(5):821-832.e1. DOI: 10.1016/j.jpainsymman.2016.12.331
[3] Rietjens JA, Sudore RL, Connolly M, van Delden JJ, Drickamer MA, Droger M, van der Heide A, Heyland DK, Houttekier D, Janssen, DJ, Orsi L, Payne S, Seymour J, Jox RJ, Korfage IJ; European Association for Palliative Care. Definition and recommendations for advance care planning: an international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017;18(9):e543-e551. DOI: 10.1016/S1470-2045(17)30582-X
[4] Götze K, Feddersen B, Marckmann G, Schildmann J, in der Schmitten J. Advance Care Planning – Annäherung an eine operationale Definition durch eine Theory-of-Change. Z Palliativmed. 2022;23(05):e30. DOI: 10.1055/s-0042-1754083
[5] Montgomery C, Anderson S, Hammes B, Briggs L. Das Respecting Choices Advance Care Planning Program: ein nachweislicher Erfolg. In: Jox RJ, Krones T, Marckmann G, in der Schmitten J, editors. Praxisbuch Advance Care Planning. Stuttgart: Kohlhammer; 2025.
[6] Goodwin J. To tatou reo - Our voice: Advance Care Planning in Aotearoa New Zealand. Z Evid Fortbild Qual Gesundhwes. 2023;180:168-173. DOI: 10.1016/j.zefq.2023.05.014
[7] Götze K, Feddersen B, in der Schmitten J, Marckmann G. Advance Care Planning in Germany. Z Evid Fortbild Qual Gesundhwes. 2023;180:127-132. DOI: 10.1016/j.zefq.2023.05.005
[8] Götze K, Bausewein C, Feddersen B, Fuchs A, Hot A, Hummers E, Icks A, Kirchner Ä, Kleinert E, Klosterhalfen S, Kolbe H, Laag S, Lagner H, Lezius S, Meyer G, Montalbo J, Nauck F, Reisinger C, Rieder N, Schildmann J, Schunk M, Stanze H, Vogel C, Wegscheider K, Zapf A, Marckmann G, in der Schmitten J; BEVOR study group. Effectiveness of a complex regional advance care planning intervention to improve care consistency with care preferences: study protocol for a multi-center, cluster-randomized controlled trial focusing on nursing home residents (BEVOR trial). Trials. 2022 Sep 12;23(1):770. DOI: 10.1186/s13063-022-06576-3
[9] Krones T, Budilivschi A, Karzig I, Otto T, Valeri F, Biller-Andorno N, Mitchell C, Loupatatzis B. Advance care planning for the severely ill in the hospital: a randomized trial. BMJ Support Palliat Care. 2019;12(e3):e411-e413. DOI: 10.1136/bmjspcare-2017-001489
[10] in der Schmitten J, Lex K, Mellert C, Rothärmel S, Wegscheider K, Marckmann G. Patientenverfügungsprogramm – Implementierung in Senioreneinrichtungen. Dtsch Arztebl. 2014;111(4):50-57. DOI: 10.3238/arztebl.2014.0050
[11] Clavien C, Ehlers U, R JJ, Karzig I, Krones T, Loupatzatzis B, Monteverde S, Theile G. Advance Care Planning in Switzerland: Chances and challenges of delivering high-quality ACP in a small high-income, multilingual, federally organized country. Z Evid Fortbild Qual Gesundhwes. 2023;180:115-120. DOI: 10.1016/j.zefq.2023.04.008
[12] Sinclair C, Mann J, Reymond L, Sansome X. Advance Care Planning in Australia: Progress in research and implementation. Z Evid Fortbild Qual Gesundhwes. 2023;180:111-114. DOI: 10.1016/j.zefq.2023.05.012
[13] Peters T, Thrien C, editors. Simulationspatienten - Handbuch für die Aus- und Weiterbildung in medizinischen und Gesundheitsberufen. Bern: Hogrefe Verlag; 2018. DOI: 10.1024/85756-000
[14] Langewitz W. Breaking bad news-Quo vadis? Patient Educ Couns. 2017;100(4):607-609. DOI: 10.1016/j.pec.2017.03.002
[15] Otten T, Meier S. Advance Care Planning – mehr als eine Patientenverfügung 2.0. Rhein Arztebl. 2021;8:21.
[16] Otten T, Meier S. Advance Care Planning: Ein Fallbeispiel. Rhein Arztebl. 2021;9:22.
[17] Feddersen B, Petri S, Marckmann G, Topka H. Advance Care Planning - Behandlung im Voraus Planen in der Notfallmedizin. Notfallmed up2date. 2018;13(01):23-26. DOI: 10.1055/s-0043-118768
[18] Nauck F, Marckmann G, in der Schmitten J. Behandlung im Voraus planen – Bedeutung für die Intensiv- und Notfallmedizin [Advance Care Planning and its Relevance for Emergency and Intensive Care Medicine]. Anästhesiol Intensivmed Notfallmed Schmerzther. 2018;53(01):62-70. DOI: 10.1055/s-0042-118690
[19] in der Schmitten J, Jox RJ, Pentzek M, Marckmann G. Advance care planning by proxy in German nursing homes: Descriptive analysis and policy implications. J Am Geriatr Soc. 2021;69(8):2122-2131. DOI: 10.1111/jgs.17147
[20] Götze K, Loupatatzis B, Otten S. Von der Begegnung mit Tabus Qualifizierung von ACP-Gesprächsbegleitern. Dr Med Mabuse. 2018;236(6):34-37.
[21] Kaplonyi J, Bowles KA, Nestel D, Kiegaldie D, Maloney S, Haines T, Williams C. Understanding the impact of simulated patients on health care learners' communication skills: a systematic review. Med Educ. 2017;51(12):1209-1219. DOI: 10.1111/medu.13387
[22] King AM, Perkowski-Rogers LC, Pohl HS. Planning standardized patient programs: Case development, patient training, and costs. Teach Learn Med. 1994;6(1):6-14. DOI: 10.1080/10401339409539636
[23] Hunt EA, Duval-Arnould JM, Nelson-McMillan KL, Bradshaw JH, Diener-West M, Perretta JS, Shilkofski NA. Pediatric resident resuscitation skills improve after "rapid cycle deliberate practice" training. Resuscitation. 2014;85(7):945-591. DOI: 10.1016/j.resuscitation.2014.02.025
[24] Adamo G. Simulated and standardized patients in OSCEs: achievements and challenges 1992-2003. Med Teach. 2003;25(3):262-270. DOI: 10.1080/0142159031000100300
[25] Barrows HS. Simulated (standardized) Patients and Other Human Simulations. Owasso (OK): National Consortium for Health Science Education; 1987.
[26] Stanislawski KS. Stanislawski - Die Arbeit des Schauspielers an sich selbst. 6. Aufl. Leipzig: Henschel Verlag; 2002.
[27] Batson S. TRUTH Wahrhaftigkeit im Schauspiel - Ein Lehrbuch. Berlin: Alexander Verlag; 2017.
[28] Wallace P. Coaching Standardized Patients for Use in the Assessment of Clinical Competence. 1st edition. New York: Springer Publishing Company; 2007.
[29] Stegemann B. Lektionen 3. Schauspielen. Theorie. Berlin: Theater der Zeit; 2010.
[30] Roselt J, editor. Regie im Theater. Geschichte – Theorie – Praxis. Berlin: Alexander Verlag; 1983.
[31] Taras J, Everett T. Rapid Cycle Deliberate Practice in Medical Education - a Systematic Review. Cureus. 2017;9(4):e1180. DOI: 10.7759/cureus.1180
[32] Ng C, Primiani N, Orchanian-Cheff A. Rapid Cycle Deliberate Practice in Healthcare Simulation: a Scoping Review. Med Sci Educ. 2021;31(6):2105-2120. DOI: 10.1007/s40670-021-01446-0
[33] Petri S, Götze K, Feddersen B. Train the Trainer - Qualifizierung von Trainern für BVP-Gesprächsbegleiter. Palliativ Pflegen. 2019;43:14-15.
[34] Feddersen B, Götze K, in der Schmitten J. Qualifizierung von ACP-Gesprächsbegleiter-Trainern. In: Jox RJ, Krones T, Marckmann G, in der Schmitten J, editors. Praxisbuch Advance Care Planning. Stuttgart: Kohlhammer; 2024.
[35] Götze K, Otten-Marré S, Loupatatzis B, in der Schmitten J. Entwicklung komplexer Gesprächskompetenzen für Advance Care Planning durch Simulationspersonen-gestütztes Training. In: Jox R, Krones T, Marckmann G, in der Schmitten J, editors. Praxisbuch Advance Care Planning. Behandlungsentscheidungen gemeinsam vorausplanen. Stuttgart: Kohlhammer; 2025.
[36] Götze K, in der Schmitten J. Abschlussbericht 06/2016 – 10/2018 Förderung der Umsetzung des §132g SGB V gemäß HPG Fkz. ZMVI1-2516FSB801. Düsseldorf: Heinrich-Heine-Universität Düsseldorf; 2019.

