“You’re a trainee telling your consultant to hold their question until later“: Using a resident-led faculty development workshop to explore trainee-consultant expertise role-reversal
Beatrice B. Preti 1,2Claire P. Browne 3
Michael S. Sanatani 1
Christopher J. Watling 1
1 Western University, Department of Oncology, London (ON), Canada
2 Emory University, Department of Haematology & Medical Oncology, Atlanta (GA), USA
3 Western University, Schulich School of Medicine & Dentistry, London (ON), Canada
Abstract
Background: Medical education traditionally involves directional flow of knowledge/skills/attitudes from a senior to junior individual. However, medical training also provides opportunities for expertise role-reversal, where the direction of flow is reversed. Unlike fields such as aviation, medicine has not yet begun to fully realise the educational potential of this approach.
Objective: To better understand how role-reversal is viewed by medical education participants, necessary for its use as a tool to advance both education and patient care.
Methods: A senior resident designed and led a feedback-writing workshop for her own consultants (conducted 2022). After the session, eight consultants were interviewed in a semi-structured format. Analysis was conducted using the Stenfors-Hayes phenomenographical approach.
Results: A multiplicity of experiential perspectives was identified by both consultants (teacher/participant/supporter/hierarchy member/colleague/holder of multiple perspectives) and trainee (presenter/subordinate/learner/researcher). The exercise increased appreciation and awareness of the complexity of the trainee-consultant educational-power relationship, though both parties maintained traditional hierarchy despite altered informational flow. Participants often held multiple articulated experiential perspectives simultaneously.
Conclusions: Consultants were able to assume a learning mindset while simultaneously maintaining awareness of their existing hierarchical relationship to the trainee-presenter; the trainee, conversely, struggled to adopt the teacher mindset. Deliberately viewing moments where trainees present new information to consultants as expertise role-reversal may provide a starting point for more equitable knowledge exchange between both parties in the clinical routine, and a foil for epistemic injustice. Increasing recognition and use of expertise role reversal can play a critical role in improving educational culture.
Keywords
medical education, continuing professional development, role reversal, phenomenography
1. Introduction
Written feedback in medical education ideally provides essential instructions for growth, as well as formalising a record of learning. However, the feedback often varies in quality [1], which subsequently influences its utility in enhancing a learner’s performance/skillset. There have been numerous interventions documented in the literature aimed at improving the quality of written feedback; however, these have been lukewarm in their successes, with a number of limitations, ranging from feasibility and buy-in to tangible improvement [2], [3].
Despite longstanding calls for feedback to be dialogic and conversational [4], [5], it typically continues to involve a directional flow of knowledge, skills, or attitudes from a senior to a junior individual. However, scenarios in medicine where the traditional directional flow is modified have been established. Such situations include co-learning, where trainees and consultants learn together to address a mutual knowledge gap [6], or reverse mentoring, where a more junior mentee provides new, fresh insights and guidance to an older mentor [7]. Both of these models highlight alternatives to the traditional directional flow of medical education, providing options for informational flow and, consequently, knowledge acquisition for all members of the team, which could benefit team members’ own learning as well as task accomplishment. Conversely, instances of so-termed “epistemic injustice”, have also been well-documented in the literature [8]. Epistemic injustice is a negative psychological reaction to unrecognised expertise role-reversal and may be triggered by a devaluation or failure to acknowledge a more junior individual’s contributions or knowledge. Epistemic injustice and its sequelae, including moral distress and weakening of the trainee-consultant relationship, are acknowledged in various healthcare professionals, but have serious implications when considered in the trainee (future healthcare professional) populations, including decreased retention in the field, increased burnout, and decreased job satisfaction [8], [9], [10], [11].
Instances of complete reversal of insights, guidance, and/or knowledge (from junior to senior) are more commonly embraced in fields outside medicine. In aviation, junior individuals freely provide suggestions and advice to more senior individuals [12]. This practice forms an essential part of “crew resource management”, a form of emergency management that consciously rejects hierarchical norms and utilizes all available expertise [13]. While this may be seen as a focus on psychological safety (the learner feels safe speaking up) [14], as well as expertise role-reversal, the contribution of the junior individual has to be deliberately recognised for successful knowledge transfer. This allows for innovation and teamwork aimed towards optimal outcomes in unusual or high-risk/high-stress situations. As another profession where decisions may have severe consequences and, therefore, clear-eyed decision-making is necessary, medical education can learn much from aviation in how to facilitate knowledge sharing [12]. Indeed, enhancing teamwork through deliberate training of learners’ speaking up skills, and supervisors’ own feedback receptivity, is an ongoing educational strategy [15], [16].
The improvement of written feedback provides a natural opportunity to consider utilising an expertise role-reversal approach in medicine. As direct recipients and beneficiaries of faculty feedback, trainees are in an ideal position to coach faculty members on ways to improve written feedback. One method previously trialled in higher education to address the issues surrounding subpar feedback is a reversed-role faculty development session, during which learners provide instruction to faculty [17]. This is a strategy we seek to explore further within medical education, where individuals in traditional “student” roles lead faculty development sessions instructing their teachers on how to provide optimal feedback.
It is essential to acknowledge that hierarchies inherent to medicine (and the hidden curriculum) might cause some trainees to balk at the prospect of teaching their superiors, or cause some faculty to distrust an educational presentation by their subordinates. Exploring these feelings is essential to understand the feasibility of expertise role-reversal scenarios and identify potential barriers to broader implementation.
Consequently, we conducted a resident-led feedback writing workshop grounded in expertise-role reversal, with the goal to understand how the session was experienced by participants.
2. Methods
Given our goal of exploring the social experience of a role-reversed educational activity, a qualitative research approach was chosen. Within a constructivist epistemology, phenomenography was chosen as the specific methodology. Phenomenography refers to a research approach in which small snippets of described experience are used to build a holistic picture of a situation [18], including individual variations in the experienced situation, from the perspective of those experiencing the situation [19]. This was an appealing methodology as we were focused on understanding the possible broad landscape of faculty members’ responses and lived experiences of the phenomenon of a trainee-led workshop. The research paradigm involved a relativist ontology (reality is based on individual experiences), constructivist epistemology (knowledge of reality is constructed by individuals), and constructivist paradigm (individuals construct reality through their perceptions of the world around them).
The faculty development session itself consisted of a single-session, in-person workshop aimed at medical oncologists in a tertiary-care academic centre in Ontario. The session was designed and led in 2022 by a then-fifth-year medical oncology trainee (BP) at the same centre as faculty members MS and CJW, and based on Gagne’s model of instructional design [20]. The workshop lasted two hours; the first half was didactic with interactive built-in questions, and the second half involved simulated feedback scenarios with a standardised student. Oncologists were recruited in advance of the session for participation in the study; workshop participation without study participation was also permitted. Shortly after the session, consenting faculty members (n=8) participated in a short, semi-structured, face-to-face interview (see figure 1 [Fig. 1]). Interviews were conducted by a dedicated then-non-oncologist, non-workshop-participant physician (CB) who received training in qualitative interviewing, and then recorded and transcribed using transcription software, with a manual check (see table 1 [Tab. 1]). One participating faculty member (MS) was a member of the study team. An interview was also conducted by CB with the trainee presenter using the same approach.
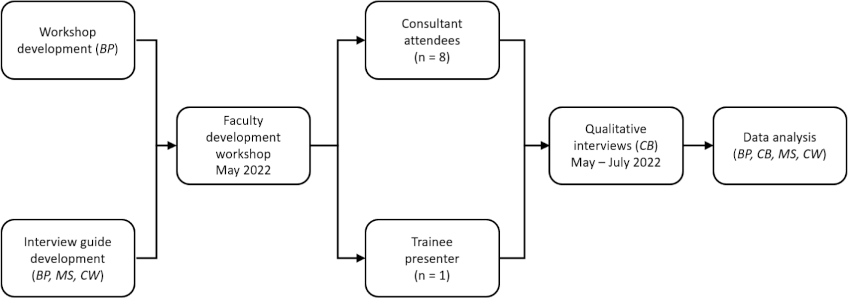
Table 1: Faculty semi-structured interview prompt questions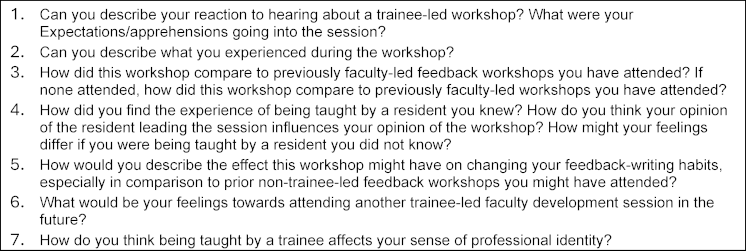
Analysis was conducted in accordance with the framework laid out by Stenfors-Hayes [21]. Following transcription, inductive coding was performed; codes were then grouped into categories to explain the experience of expertise role-reversal in the context of a trainee-led workshop. A member check was performed after initial coding by sending a copy to participants to ensure their perspectives had been accurately captured. An audit trail was also kept by the first author to assist with study confirmability and dependability [22]. Analyses were reviewed and agreed upon by all team members.
This study received ethics approval from the western research ethics board.
3. Results
3.1. Consultant roles
Seven experiential perspectives were identified by consultant participants during the workshop. These highlighted the ability of consultants to place themselves in the role of a learner when they felt this mindset might be of benefit, yet simultaneously maintain other roles, some of which were more natural or typical for the consultant. The seven experiential perspectives identified by participants were:
3.1.1. Perspective #1: Consultant as a teacher/mentor/coach of trainees in general
The session was seen as a good opportunity for any trainee, both to practice presenting and to demonstrate knowledge in the content area. Consultant attendees were also interested in the session topic and appreciated learning about ways to improve their teaching skills. They saw room for improvement in their own feedback practices (most were highly motivated to attend session based on content alone).
3.1.2. Perspective #2: Consultant as a participant in a faculty development session
Generally positive feedback towards session content and delivery was conveyed, with particular emphasis on the trainee’s presentation style and skill. Some feedback was constructive, such as lack of humour during the presentation, or a sense of distraction from exaggerated demonstrations. The workshop itself was positively received and seen as effective, and specific learning points were remembered and discussed. The trainee presenter, as a senior trainee and a trainee in the consultants’ own division, was seen as particularly credible, which also contributed to session buy-in. Pre-existing knowledge of and relationship with the trainee, and knowledge of trainee’s interests and training in education, also influenced the experience by adding further interest in/buy-in to the session. More broadly speaking, participants voiced enthusiasm at attending another trainee-led session in the future, but some were conflicted on whether trainees could teach scientific or medical content (whether alone or with consultant guidance), as consultants are the content experts in these fields. Consultants also commented on the trainee’s credibility, citing prior knowledge of the trainee which increased credibility, as well as conveying scepticism about a session led by a trainee with less credibility.
3.1.3. Perspective #3: Consultant as an empathetic supporter of the trainee
Participants reported concern for the specific trainee and for generic trainees in positions of teaching their own consultants. Consultant support for a trainee leading a session was felt to be mandatory, although no consultants were involved in session preparation or execution. Simultaneously, it was noted by participants that the trainee was receiving tacit support from a mentor in the audience during the presentation. Concern for the specific trainee was noted by quite a few participants, citing presumption or knowledge of the trainee’s anxiety or intimidation leading the session. Simultaneously, however, consultants were pleased for the trainee to have opportunity to present, and to have done so well.
3.1.4. Perspective #4: Consultant as a researcher
Participants noted reflecting on the session, both during the session and afterwards, in anticipation of interview. They also noted that comfort/effectiveness of trainee-led workshop would depend on the specific trainee, consultants, and setting; not every trainee can present every topic to every group (again relating to trainee credibility). Comparisons normalising the experience were made to patient-reported data, and that a trainee presenting trainee experience or a medical education topic is similar to a patient presenting patient experience. This, again, serves as a foil to a trainee presenting in an area where a consultant is seen as an expert.
3.1.5. Perspective #5: Consultant as a member of an existing hierarchical structure/assessor of trainee
Several consultants described seeing the senior trainee as closer to a colleague than a trainee, which impacted their experience of the session as “trainee-led”. Indeed, the opinion of workshop seems largely shaped by the opinion of the trainee, and the perceived credibility of the trainee seemed to play largely into the workshop experience.
Participants did note that some consultants might take umbrage to being taught by a trainee, and some expressed skepticism at being taught by more junior or less credible learners. Indeed, credibility of the trainee presenter was discussed by many participants, with factors such as formal training in education, interest in the field, and personal knowledge of the trainee’s skills lending credibility. It was recognised that the direction of informational flow was reversed during the workshop, but consultants felt that the hierarchy was still maintained. The session was viewed as a performance by a trainee towards consultants, similar to a case presentation in a clinical session. Awareness of a traditional culture of power or hierarchy between consultants and learners was also mentioned. Some consultants proposed breaking down the hierarchy for freer exchange of ideas/information between consultants and trainees. In general, however, consultants highlighted an increased appreciation of the complexity of the trainee-consultant educational and power relationship after the workshop.
3.1.6. Perspective #6: Consultant as a colleague of other audience members
Pre-existing collegial relationships influenced interpretation of room’s atmosphere and general awareness of the room. For example, interruptions from colleagues were appreciated by consultants who were hoping for humour or distraction during drier parts of the workshop.
It was also noted that a multitude of perspectives might work best to engage the faculty in the room:
3.1.7. Perspective #7: Consultant as a holder of multiple articulated perspectives
Consultants reported feeling conflicted during the workshop and becoming aware of possessing multiple, simultaneously-articulated perspectives, such as empathising with the trainee presenter while being interested in session content, or being anxious/guilty on behalf of the trainee and proud of the trainee. Consultants described putting themselves in the trainee’s shoes, switching in-and-out of a teacher or participant role and more into an empathetic supporter role. A dichotomy was explicitly described between the consultant as a learner and as an assessor of the trainee during the session. Consultants described switching between roles deliberately to handle moments of vulnerability, as well as occasionally feeling unsettled when trying to reconcile conflicting, equally-significant roles.
3.2. Trainee roles
Four experiential perspectives were identified by the trainee leading the workshop. These were:
3.2.1. Perspective #1: Trainee as a presenter/teacher
The trainee engaged in extensive, intense preparation for the session, representing in retrospect a response to her discomfort with teaching her own consultants. Session design and preparation were constructed, in part, to maintain control of the room; a didactic teaching style and highly-structured mode of audience interaction were anticipated to help project authority and facilitate the reversed information flow. Maintaining control of the room’s dynamic and presentation structure was used to mitigate fear, anxiety, and insecurity around teaching the trainee’s own consultants. Reflection revealed that both the trainee’s preparation intensity and her own negativity towards interactivity/spontaneity was driven by anxiety and discomfort.
3.2.2. Perspective #2: Trainee as a subordinate in a medical hierarchy
The trainee voiced repeated anxieties and insecurities related to teaching her own consultants; respected consultants were described as ultimate authority figures, and she voiced concerns about meeting expectations, despite the novel nature (and consequent lack of expectations) of the teaching structure. She also cited concerns about perception of credibility, and deliberately selected a workshop topic and angle to maximise credibility, as well as designing the talk to reflect the opinions of many trainees (not just hers, which was emphasised multiple times). The trainee reflected on expecting negative response to the workshop, and was surprised by positive responses and feedback to the workshop, which was seen as validating and supportive by those with more experience/in higher positions.
3.2.3. Perspective #3: Trainee as a learner in a teaching programme
The trainee was in a performance mindset during the preparation for and execution of the workshop, and, again, voiced repeated concerns about fulfilling consultant expectations. It was also clear that the trainee had pre-existing relationships with and perspectives of different audience members, which also influenced both anxieties and development/presentation of the workshop.
3.2.4. Perspective #4: Trainee as a researcher
The trainee also had awareness of multiple experiences in the moment. For example, the trainee reflected on duality as a researcher answering a question versus an individual delivering a judged performance to her own consultants.
3.3. Participant learning
Although not the primary focus of this study, it should be noted that faculty recalled several salient points they had learned, suggesting the session was effective. During the interviews, consultants were able to recall key learning points which had influenced their feedback writing practice, including several feedback structures discussed, deliberate word choice, and focusing on the trainee’s mindset and feedback receptivity in the moment. They appreciated the trainee perspective around written feedback, because some more senior faculty had not personally experienced receiving the type of constructive feedback they were now expected to provide.
4. Discussion
In summary, this study explored the experience of participants in a workshop using expertise role-reversal to teach feedback writing. Key takeaways include the positive overall reception and perceived efficacy of the workshop by consultant participants, who were highly receptive to being taught by a trainee.
Given the established hierarchies, expectations, and cultural norms inherent to medicine [23], there was a priori concern that these conventions might prevent learning in an expertise role-reversal setting by acting as immutable and unarticulated aspects of the hidden curriculum. However, the success of this study and the participants’ reflections emphasise that expertise role-reversal is recognisable (and embraceable) by consultants. Faculty could have had concerns about being taught specifically around a core teaching skill (namely, giving feedback) by a more junior person, as this might have threatened their professional identity as an educator; however, this was embraced and even compared to patients reporting on medical topics at conferences and seminars. Indeed, there were several references and metaphors comparing learner-led faculty development with patient involvement in care and physician education. The comparison of trainees to patients can potentially be seen as playing into existing hierarchies, where consultants can obtain information and feedback on their practices, but still remain largely in their hierarchal positions. However, analogous to increased patient autonomy and input in shared decision-making, a bidirectional, dialogue-based interaction between consultant and trainee may move education forward towards a new paradigm. In shared decision-making, physicians contribute experience around treatments and patients bring their perspectives around what matters to them [24]. Our study suggests that in the educational context, a similar sharing of educational roles may be possible. Senior physicians contribute experience around skills development, and junior physicians or trainees contribute fresh perspectives which can inform how the skills development is enacted. However, achieving this sort of dialogue requires courage and openness. Along these lines, although the trainee did report substantial anxieties and imagined negative repercussions around the workshop, she was still able to work through the discomfort of performing outside a conventional trainee-consultant relationship to deliver a well-received workshop. In other words, the trainee did perceive risk to the expertise-role reversal, but was still able to participate. However, weight of the medical hierarchy and medical culture was a strong theme in the trainee’s reflections, as well as consultant interviews.
As a single-department, single centre study, our results are strongly influenced by the existing culture in the department, which does serve as a limitation of the study. The openness of consultants towards learning from their trainees will likely be influenced strongly by existing traditions, which will vary from one department to the next, even within the same institution. Similarly, trainees will vary widely in their experienced psychological safety when interacting with the same group of consultants, depending on their own developing professional and personal identities, as well as personality, prior experiences, and dynamics in the moment. Nonetheless, elements of the experiences of both trainees and consultants in our study would possibly be found to varying degrees if the study were to be repeated with other individuals. Further research confirming the essential experience domains we identified is encouraged.
Based on the positive reception of and feedback for the trainee-led faculty development session, we hope that this mode of teaching might be used and explored further, especially in the context of medical education faculty development. As end-users of medical education, trainees are in an ideal place to provide education to faculty members regarding educational practices.
5. Conclusion
In summary, we have presented a feedback-writing workshop designed and led by a trainee; this was well received by consultants, who were able to assume a learning mindset while simultaneously being aware of their existing hierarchical relationship to the presenting trainee. It was more difficult for the trainee to overcome concerns related to pre-existing fears and anxieties and to view herself primarily as a teacher, suggesting that such concerns must be deliberately addressed as well, in order for a bidirectional information flow to occur in clinical settings. However, deliberately viewing moments where a trainee is presenting information that is not known (and can’t be known) by the consultant at that point in time may serve as a starting point for more equitable exchange of knowledge between trainees and consultants in the clinical routine
Authors’ ORCIDs
- Beatrice Preti: [0000-0002-3664-417X]
- Michael Sanatani: [0000-0002-2423-7171]
- Christopher Watling: [0000-0002-1440-2401]
Competing interests
The authors declare that they have no competing interests.
References
[1] Dehmoobad Sharifabadi A, Clarkin C, Doja A. Perceptions of competency-based medical education from medical student discussion forums. Med Educ. 2019;53(7):666-676. DOI: 10.1111/medu.13803[2] Sanatani M, Potvin K, Conter H, Trudgeon K, Warner A. Quality of written feedback given to medical students after introduction of real-time audio monitoring of clinical encounters. BMC Med Educ. 2020;20(1):236. DOI: 10.1186/s12909-020-02158-6
[3] Zelenski AB, Tischendorf JS, Kessler M, Saunders S, MacDonald MM, Vogelman B, Zakowski L. Beyond “Read More”: An Intervention to Improve Faculty Written Feedback to Learners. J Grad Med Educ. 2019;11(4):468-471. DOI: 10.4300/JGME-D-19-00058.1
[4] Watling C, Driessen E, van der Vleuten CP, Lingard L. Learning culture and feedback: An international study of medical athletes and musicians. Med Educ. 2014;48(7):713-723. DOI: 10.1111/medu.12407
[5] Miles A, Ginsburg S, Sibbald M, Tavares W, Watling C, Stroud L. Feedback from health professionals in postgraduate medical education: Influence of interprofessional relationship, identity and power. Med Educ. 2021;55(4):518-529. DOI: 10.1111/medu.14426
[6] Haddock L, Rivera J, O’Brien BC. Learning Together: Co-Learning Among Faculty and Trainees in the Clinical Workplace. Acad Med. 2023;98(2):228-236. DOI: 10.1097/ACM.0000000000004836
[7] Clarke AJ, Burgess A, van Diggele C, Mellis C. The role of reverse mentoring in medical education: Current insights. Adv Med Educ Pract. 2019;10:693-701. DOI: 10.2147/AMEP.S179303
[8] Carel H, Kidd IJ. Epistemic injustice in healthcare: a philosophial analysis. Med Health Care Philos. 2014;17(4):529-540. DOI: 10.1007/s11019-014-9560-2
[9] Dunne G. Epistemic injustice in education. Educ Phil Theor. 2023;55(3):285-289. DOI: 10.1080/00131857.2022.2139238
[10] Consejo C, Viesca CA. Injusticia epistémica durante el proceso de formación médica en el contexto hospitalario [Epistemic injustice during the medical education process in the hospital context]. Rev Med Inst Mex Seguro Soc. 2017;55(3):400-408.
[11] Reed PG, Rishel CJ. Epistemic Injustice and Nurse Moral Distress: Perspective for Policy Development. Nurs Sci Q. 2015;28(3):241-244. DOI: 10.1177/0894318415585634
[12] Singh N. On a wing and a prayer: Surgeons learning from the aviation industry. J R Soc Med. 2009;102(9):360-364. DOI: 10.1258/jrsm.2009.090139
[13] Sexton B, Thomas E, Helmreich RL. Error, stress, and teamwork in medicine and aviation: Cross sectional surveys. BMJ. 2000;320(7237):745-749. DOI: 10.1136/bmj.320.7237.745
[14] Edmondson A. Psychological safety and learning behavior in work teams. Adm Sci Q. 1999;44(2):350-383. DOI: 10.2307/2666999
[15] Kim S, Appelbaum NP, Baker N, Bajwa NM, Chu F, Pal JD, Cochran NE, Bochatay N. Patient Safety Over Power Hierarchy: A Scoping Review of Healthcare Professionals’ Speaking-up Skills Training. J Healthc Qual. 2020;42(5):249-263. DOI: 10.1097/JHQ.0000000000000257
[16] Weller JM, Long JA. Creating a climate for speaking up. Br J Anaesth. 2019;122(6):710-713. DOI: 10.1016/j.bja.2019.03.003
[17] Wright DB, Mullen A, Gardner A. Does Student-Led Faculty Development Have A Place in Health Professions Education? MedEdPublish. 2019;8:34. DOI: 10.15694/mep.2019.000034.1
[18] Forster M. “Ethnographic” thematic phenomenography: A methodological adaptation for the study of information literacy in an ontologically complex workplace. J Doc. 2019;75(2):349-365. DOI: 10.1108/JD-05-2018-0079
[19] Stolz SA. Phenomenology and phenomenography in educational research: A critique. Educ Phil Theor. 2020;52(10):1077-1096. DOI: 10.1080/00131857.2020.1724088
[20] Lo WL, Hsieh MC. Teaching communication skills: Using Gagne’s model as an illustration. Ci Ji Yi Xue Za Zhi. 2019;32(1):19-25. DOI: 10.4103/tcmj.tcmj_59_19
[21] Stenfors-Hayes T, Hult H, Dahlgren MA. A phenomenographic approach to research in medical education. Med Educ. 2013;47(3):261-270. DOI: 10.1111/medu.12101
[22] Amin MEK, Nørgaard LS, Cavaco AM, Witry MJ, Hillman L, Cernasev A, Desselle SP. Establishing trustworthiness and authenticity in qualitative pharmacy research. Res Soc Adm Pharm. 2020;16(10):1472-1482. DOI: 10.1016/j.sapharm.2020.02.005
[23] Salehi PP, Jacobs D, Suhail-Sindhu T, Judson BL, Azizzadeh B, Lee YH. Consequences of Medical Hierarchy on Medical Students, Residents, and Medical Education in Otolaryngology. Otolaryngology Head Neck Surg. 2020;163(5):906-914. DOI: 10.1177/0194599820926105
[24] Epstein RM, Street RL. Shared mind: Communication, decision making, and autonomy in serious illness. Ann Fam Med. 2011;9(5):454-461. DOI: 10.1370/afm.1301

